

Why has it been so difficult to prove the efficacy of alpha-1-antitrypsin replacement therapy? Insights from the study of disease pathogenesis
- PMID: 21966212
- PMCID: PMC3180514
- DOI: 10.2147/DDDT.S14018
Why has it been so difficult to prove the efficacy of alpha-1-antitrypsin replacement therapy? Insights from the study of disease pathogenesis
Abstract
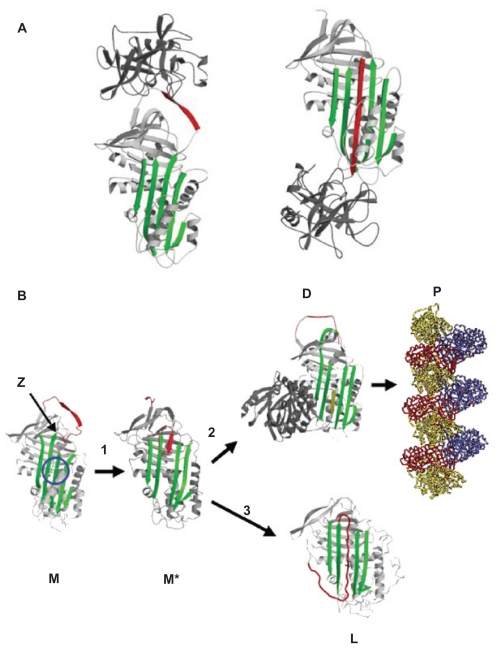
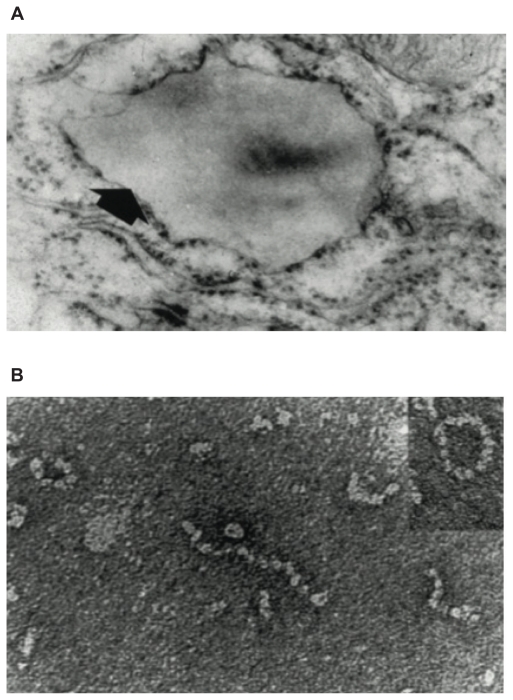
Alpha-1-antitrypsin is the most abundant circulating protease inhibitor. It is mainly produced by the liver and secreted into the circulation where it acts to prevent excessive proteolytic damage in the lungs by the enzyme neutrophil elastase. The most common severe deficiency allele is the Z mutation, which causes the protein to self-associate into ordered polymers. These polymers accumulate within hepatocytes to cause liver damage. The resulting lack of circulating α(1)-antitrypsin predisposes the Z homozygote to proteolytic lung damage and emphysema. Other pathways may also contribute to the development of lung disease. In particular, polymers of Z α(1)-antitrypsin can form within the lung where they act as a pro-inflammatory stimulus that may exacerbate protease-mediated lung damage. Researchers recognized in the 1980s that plasma α(1)-antitrypsin levels could be restored by intravenous infusions of purified human protein. Alpha-1-antitrypsin replacement therapy was introduced in 1987 but subsequent clinical trials have produced conflicting results, and to date there remains no widely accepted clinical evidence of the efficacy of α(1)-antitrypsin replacement therapy. This review addresses our current understanding of disease pathogenesis in α(1)-antitrypsin deficiency and questions why this treatment in isolation may not be effective. In particular it discusses the possible role of α(1)-antitrypsin polymers in exacerbating intrapulmonary inflammation and attenuating the efficacy of α(1)-antitrypsin replacement therapy.
Keywords: augmentation therapy; emphysema; α1-antitrypsin deficiency.
Figures
References
-
- Laurell C-B, Eriksson S. The electrophoretic α1-globulin pattern of serum in α1-antitrypsin deficiency. Scand J Clin Lab Invest. 1963;15:132–140. - PubMed
-
- Sharp HL, Bridges RA, Krivit W, Freier EF. Cirrhosis associated with alpha-1-antitrypsin deficiency: a previously unrecognized inherited disorder. J Lab Clin Med. 1969;73(6):934–939. - PubMed
-
- King MA, Stone JA, Diaz PT, et al. α1-antitrypsin deficiency: evaluation of bronchiectasis with CT. Radiology. 1996;199(1):137–141. - PubMed
-
- Eden E, Mitchell D, Mehlman B, et al. Atopy, asthma, and emphysema in patients with severe alpha-1-antitrypsin deficiency. Am J Respir Crit Care Med. 1997;156(1):68–74. - PubMed
-
- Griffith ME, Lovegrove JU, Gaskin G, Whitehouse DB, Pusey CD. C-anti-neutrophil cytoplasmic antibody positivity in vasculitis patients is associated with the Z allele of alpha-1-antitrypsin, and the P-antineutrophil cytoplasmic antibody positivity with the S allele. Nephrol Dial Transplant. 1996;11(3):438–443. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
