

Does the Pirani score predict relapse in clubfoot?
- PMID: 21966308
- PMCID: PMC2946533
- DOI: 10.1007/s11832-010-0287-1
Does the Pirani score predict relapse in clubfoot?
Abstract
Purpose: Presented here is a retrospective clinical audit of clubfoot patients to determine the value of the Pirani clubfoot scoring system at initial presentation in the estimation of subsequent relapse.
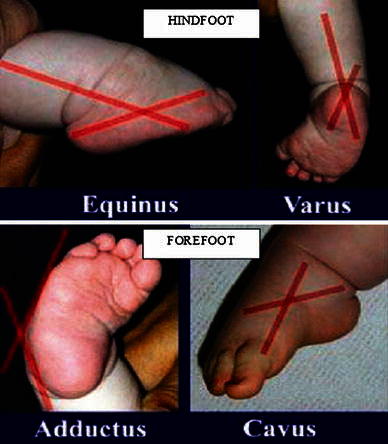
Methods: All clubfoot patients treated by the same surgeon from 2002 to 2006 were included. The treatment adhered to the standard protocol, involving weekly stretching and casting until the foot was corrected, followed by Achilles tenotomy and plasters for 3 weeks. Thereafter, the child was placed in a foot abduction splint. The severity of clubfoot was assessed using the Pirani scoring system, consisting of two sub-scores-the midfoot contracture score (MFCS) and the hindfoot contracture score (HFCS). The MFCS and HFCS can each be 0.0-3.0, giving rise to a total Pirani score (TPS) of 0.0-6.0. Any recurrent deformity was classed as a relapse.
Results: Sixty-one clubfoot patients were treated. Five patients were lost to follow-up and six patients were excluded due to the presence of identified syndromes or having had primary treatment elsewhere. A total of 80 clubfeet were included. There were 17 relapses. The average interval between the initiation of foot abduction splint and relapse was 23 months. The median TPS was 3.5 in the no relapse group and 5.0 in the relapse group. The median MFCS was 1.5 in the no relapse group and 2.0 in the relapse group. The median HFCS was 2.0 in the no relapse group and 3.0 in the relapse group. Higher TPS and HFCS were statistically significant when the relapse group was analysed against the no relapse group (P = 0.05 × 10(-4) and 0.02 × 10(-4), respectively).
Conclusions: Higher Pirani scores were associated with the late relapse group. The TPS and HFCS were shown to be statistically significant predictors of potential relapse. Closer follow-up is advised for patients at risk of relapse.
Keywords: Clubfoot; Pirani score; Ponseti treatment method; Relapse.
Figures




References
-
- Ponseti IV. Current concepts review: treatment of congenital club foot. J Bone J Surg Am. 1992;74(3):448–454. - PubMed
-
- Dobbs MB, Rudzki JR, Purcell DB, et al. Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J Bone J Surg Am. 2004;86-A(1):22–27. - PubMed
-
- Laaveg SJ, Ponseti IV. Long-term results of treatment of congenital club foot. J Bone J Surg Am. 1980;62-A:23–31. - PubMed
-
- Ponseti IV, Smoley EN. Congenital club foot: the results of treatment. J Bone J Surg Am. 1963;45-A:261–275.
LinkOut - more resources
Full Text Sources
