

A scoring model based on neutrophil to lymphocyte ratio predicts recurrence of HBV-associated hepatocellular carcinoma after liver transplantation
- PMID: 21966488
- PMCID: PMC3180380
- DOI: 10.1371/journal.pone.0025295
A scoring model based on neutrophil to lymphocyte ratio predicts recurrence of HBV-associated hepatocellular carcinoma after liver transplantation
Retraction in
-
Retraction: A Scoring Model Based on Neutrophil to Lymphocyte Ratio Predicts Recurrence of HBV-Associated Hepatocellular Carcinoma after Liver Transplantation.PLoS One. 2019 Jul 23;14(7):e0220418. doi: 10.1371/journal.pone.0220418. eCollection 2019. PLoS One. 2019. PMID: 31335902 Free PMC article. No abstract available.
Abstract
Background: Neutrophil to lymphocyte ratio (NLR) has been proposed to predict prognosis of hepatocellular carcinoma (HCC). However, the cut-off values are empirical. We determined the optimal cut-off value to predict HCC recurrence after liver transplantation (LT) and further established a scoring model based on NLR.
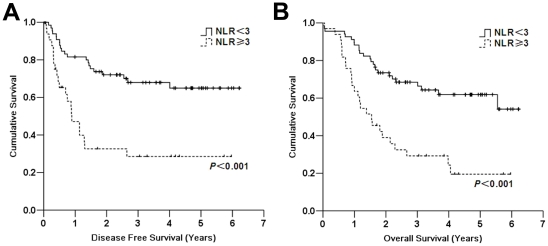
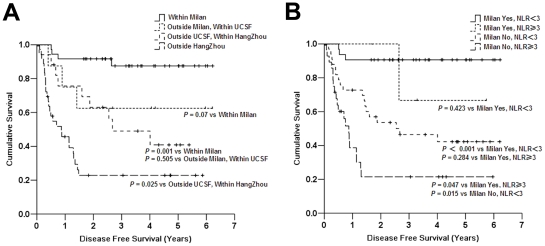
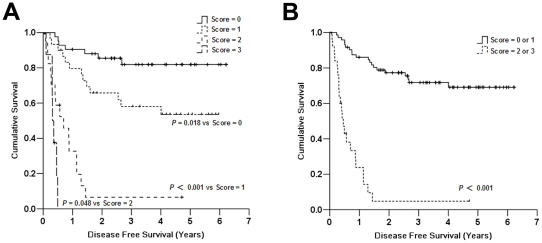
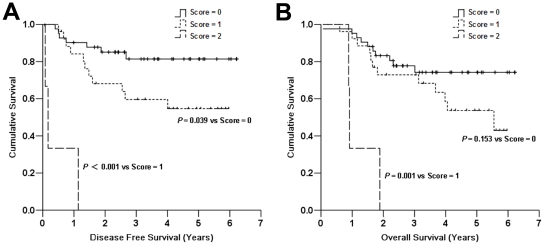
Methodology/principal findings: We analyzed the outcome of 101 HBV-associated HCC patients undergoing LT. Preoperative risk factors for tumor recurrence were evaluated by univariate analysis. By using ROC analysis, NLR≥3 was considered elevated. The disease-free survival (DFS) and overall survival (OS) for patients with high NLR was significantly worse than that for patients with normal NLR (the 5-year DFS and OS of 28.5% and 19.5% vs. 64.9% and 61.8%, respectively; P<0.001). Univariate analysis revealed that tumor size >5 cm, tumor number >3, macrovascular invasion, AFP≥400 µg/L, NLR≥3, and HBV-DNA level >5 log10 copies/mL were preoperative predictors of DFS. Cox regression analysis showed macrovascular invasion, tumor number, and high NLR were independent prognostic factors. We then established a preoperative prognostic score based on multivariate analysis. Each factor was given a score of 1. Area under the ROC curve of the score was 0.781. All nine patients with score 3 developed recurrence within 6 months after LT. Of 71 patients without vascular invasion, three patients with both tumor number >3 and NLR≥3 developed recurrence within 14 months after LT while the 5-year DFS and OS for patients with a score of 0 or 1 were 68.1% and 62.8%, respectively.
Conclusions/significance: Preoperative elevated NLR significantly increases the risk of recurrence in patients underwent LT for HCC. Patients with both NLR≥3 and tumor number >3 are not a good indication for LT. Our score model may aid in the selection of patients that would most benefit from transplantation for HCC.
Conflict of interest statement
Figures
References
-
- Chen GH. Liver transplantation in China: retrospect and prospect. Chin Med J (Engl) 2009;122:2229–30. - PubMed
-
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–9. - PubMed
-
- Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33:1394–403. - PubMed
-
- Rahbari NN, Mehrabi A, Mollberg NM, Muller SA, Koch M, et al. Hepatocellular carcinoma: current management and perspectives for the future. Ann Surg. 2011;253:453–69. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
