

Contribution of chronic disease to the burden of disability
- PMID: 21966497
- PMCID: PMC3178640
- DOI: 10.1371/journal.pone.0025325
Contribution of chronic disease to the burden of disability
Abstract
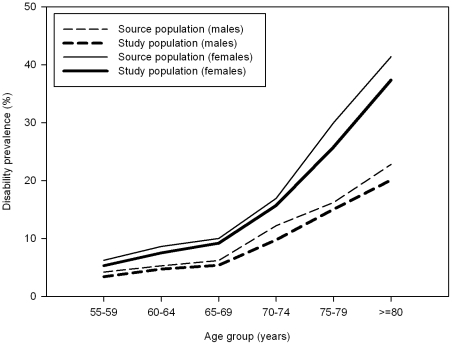
Background: Population ageing is expected to lead to strong increases in the number of persons with one or more disabilities, which may result in substantial declines in the quality of life. To reduce the burden of disability and to prevent concomitant declines in the quality of life, one of the first steps is to establish which diseases contribute most to the burden. Therefore, this paper aims to determine the contribution of specific diseases to the prevalence of disability and to years lived with disability, and to assess whether large contributions are due to a high disease prevalence or a high disabling impact.
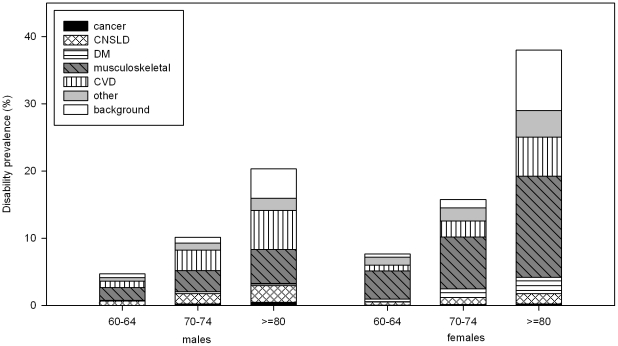
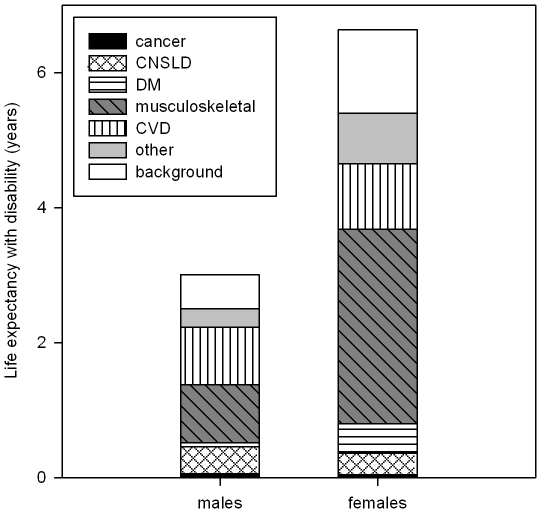
Methodology/principal findings: Data from the Dutch POLS-survey (Permanent Onderzoek Leefsituatie, 2001-2007) were analyzed. Using additive regression and accounting for co-morbidity, the disabling impact of selected chronic diseases was calculated, and the prevalence and years lived with ADL and mobility disabilities were partitioned into contributions of specific disease. Musculoskeletal and cardiovascular disease contributed most to the burden of disability, but chronic non-specific lung disease (males) and diabetes (females) also contributed much. Within the musculoskeletal and cardiovascular disease groups, back pain, peripheral vascular disease and stroke contributed particularly by their high disabling impact. Arthritis and heart disease were less disabling but contributed substantially because of their high prevalence. The disabling impact of diseases was particularly high among persons older than 80.
Conclusions/significance: To reduce the burden of disability, the extent diseases such as back pain, peripheral vascular disease and stroke lead to disability should be reduced, particularly among the oldest old. But also moderately disabling diseases with a high prevalence, such as arthritis and heart disease, should be targeted.
Conflict of interest statement
Figures
References
-
- Fried TR, Bradley EH, Williams CS, Tinetti ME. Functional disability and health care expenditures for older persons. Arch Intern Med. 2001;161:2602–2607. - PubMed
-
- Kovacs FMMDP, Abraira VP, Zamora JP, Teresa Gil del Real MMPH, Llobera JMDMPH, et al. Correlation Between Pain, Disability, and Quality of Life in Patients With Common Low Back Pain. Spine (Phila Pa 1976) 2004;29:206–210. - PubMed
-
- Mathers CD. Gains in health expectancy from the elimination of diseases among older people. Disabil Rehabil. 1999;21:211–221. - PubMed
-
- Nusselder WJ, Looman CW. Decomposition of differences in health expectancy by cause. Demography. 2004;41:315–334. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
