

Persisting right-sided chylothorax in a patient with chronic lymphocytic leukemia: a case report
- PMID: 21968097
- PMCID: PMC3204301
- DOI: 10.1186/1752-1947-5-492
Persisting right-sided chylothorax in a patient with chronic lymphocytic leukemia: a case report
Abstract
Introduction: Chylothorax caused by chronic lymphocytic leukemia is very rare and the best therapeutic approach, especially the role of modern immunochemotherapy, is not yet defined.
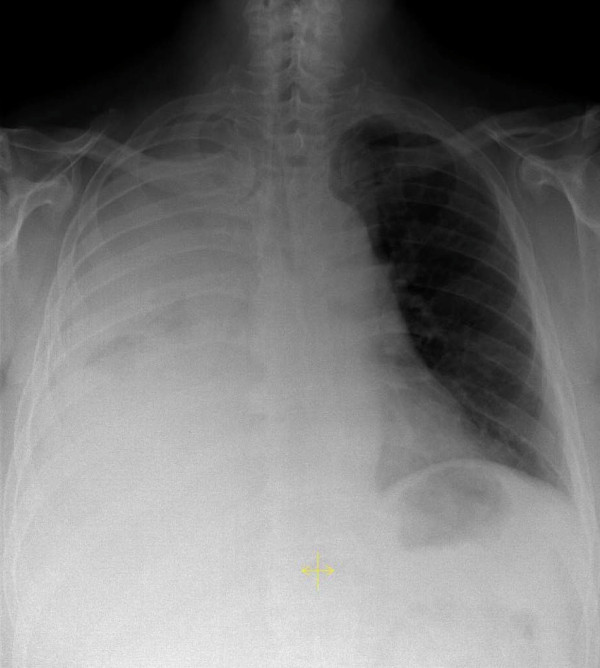
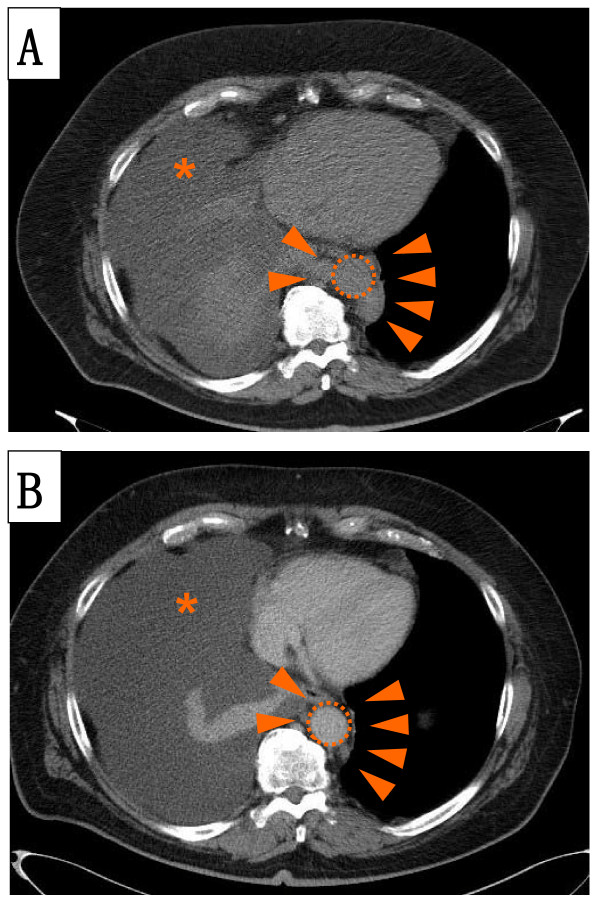
Case presentation: We present the case of a 65-year-old male Caucasian patient with right-sided chylothorax caused by a concomitantly diagnosed chronic lymphocytic leukemia. As first-line treatment four cycles of an immunochemotherapy, consisting of fludarabine, cyclophosphamide and rituximab were administered. In addition, our patient received total parenteral nutrition for the first two weeks of treatment. Despite the very good clinical response of the lymphoma to treatment, the chylothorax persisted and percutaneous radiotherapy of the thoracic duct was applied. However, eight weeks after the radiotherapy the chylothorax still persisted and our patient agreed to a surgical intervention. A ligation of the thoracic duct via a muscle sparing thoracotomy was performed, resulting in a complete cessation of the pleural effusion. Apart from the first two weeks our patient was treated on an out-patient basis for nearly six months.
Conclusion: In this case of chylothorax caused by chronic lymphocytic leukemia, immunochemotherapy in combination with conservative treatment, and even consecutive radiotherapy, were not able to stop pleural effusion, despite the very good clinical response of the chronic lymphocytic leukemia to treatment.Out-patient management using repetitive thoracocenteses can be safe as bridging until definitive surgical ligation of the thoracic duct.
Figures

References
-
- Staats BA, Ellefson RD, Budahn LL, Dines DE, Prakash UB, Offord K. The lipoprotein profile of chylous and nonchylous pleural effusions. Mayo Clin Proc. 1980;55:700–704. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
