

A pilot randomized, single-blind, placebo-controlled trial of traditional acupuncture for vasomotor symptoms and mechanistic pathways of menopause
- PMID: 21968279
- PMCID: PMC3246091
- DOI: 10.1097/gme.0b013e31821f9171
A pilot randomized, single-blind, placebo-controlled trial of traditional acupuncture for vasomotor symptoms and mechanistic pathways of menopause
Abstract
Objective: The aim of this study was to conduct a pilot study for the feasibility of planning a definitive clinical trial comparing traditional acupuncture (TA) with sham acupuncture (SA) and waiting control (WC) on menopause-related vasomotor symptoms (VMS), quality of life, and the hypothalamic-pituitary-adrenal axis in perimenopausal and postmenopausal women.
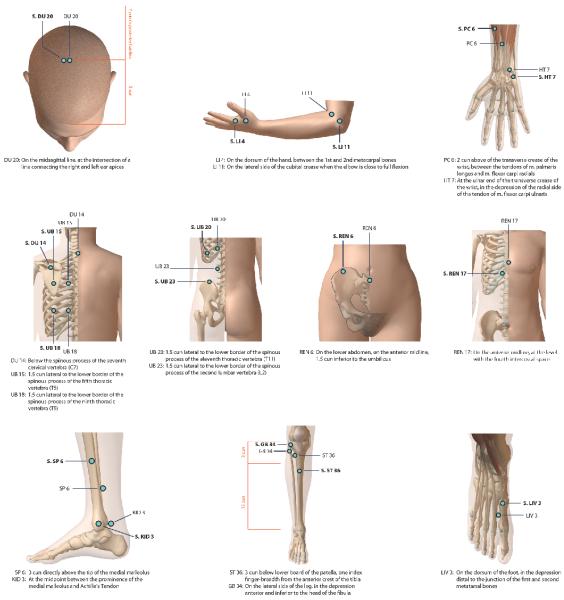
Methods: Thirty-three perimenopausal and postmenopausal women with at least seven VMS daily were randomized to TA, SA, or WC. The TA and SA groups were given three treatments per week for 12 weeks. Outcomes included the number and severity of VMS, Menopause-Specific Quality of Life Questionnaire, Beck Depression Inventory, Spielberg State-Trait Anxiety Instrument, Pittsburgh Quality Sleep Index, 24-hour urine cortisol and metabolites, and adrenocorticotropic hormone stimulation testing.
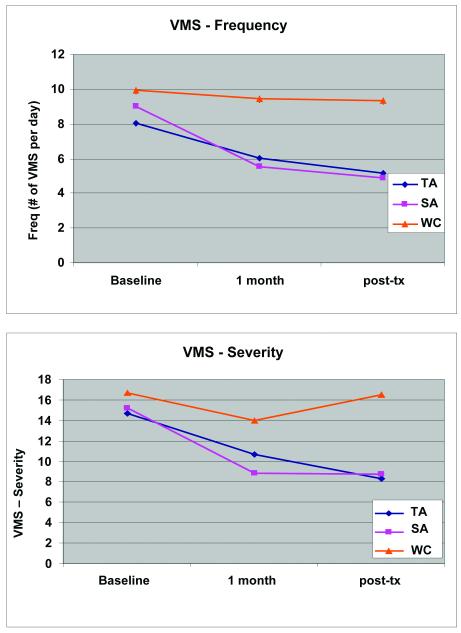
Results: Both the TA and SA groups demonstrated improved VMS trends compared with the WC group (Δ -3.5 ± 3.00 vs -4.1 ± 3.79 vs -1.2 ± 2.4, respectively; P = 20) and significantly improved Menopause-Specific Quality of Life Questionnaire vasomotor scores (Δ -1.5 ± 2.02 vs -1.8 ± 1.52 vs -0.3 ± 0.64, respectively; P = 0.04). There were no psychosocial group differences. Exit 24-hour urinary measures were lower in the TA versus the SA or WC group in total cortisol metabolites (4,658.9 ± 1,670.9 vs 7,735.8 ± 3,747.9 vs 5,166.0 ± 2,234.5, P = 0.03; respectively) and dehydroepiandrosterone (41.4 ± 27.46, 161.2 ± 222.77, and 252.4 ± 385.40, respectively; P = 0.05). The response data on adrenocorticotropic hormone stimulation cortisol also trended in the hypothesized direction (P = 0.17).
Conclusions: Both TA and SA reduce VMS frequency and severity and improve VMS-related quality of life compared with WC; however, TA alone may impact the hypothalamic-pituitary-adrenal axis. This association is viewed as preliminary and hypothesis generating and should be explored in a large clinical trial.
Trial registration: ClinicalTrials.gov NCT00950482.
Figures
References
-
- Koster A, Davidsen M. Climacteric complaints and their relation to menopausal development--a retrospective analysis. Maturitas. 1993;17:155–66. - PubMed
-
- Rabin DS, Cipparrone N, Linn ES, Moen M. Why menopausal women do not want to take hormone replacement therapy. Menopause. 1999;6:61–7. - PubMed
-
- Cauley JA, Robbins J, Chen Z, et al. Effects of estrogen plus progestin on risk of fracture and bone mineral density: the Women’s Health Initiative randomized trial. JAMA. 2003;290:1729–38. - PubMed
-
- Chlebowski RT, Hendrix SL, Langer RD, et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women’s Health Initiative Randomized Trial. JAMA. 2003;289:3243–53. - PubMed
-
- Chlebowski RT, Wactawski-Wende J, Ritenbaugh C, et al. Estrogen plus progestin and colorectal cancer in postmenopausal women. N Engl J Med. 2004;350:991–1004. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
