

Pre-operative planning for mandibular reconstruction - a full digital planning workflow resulting in a patient specific reconstruction
- PMID: 21968330
- PMCID: PMC3195208
- DOI: 10.1186/1758-3284-3-45
Pre-operative planning for mandibular reconstruction - a full digital planning workflow resulting in a patient specific reconstruction
Abstract
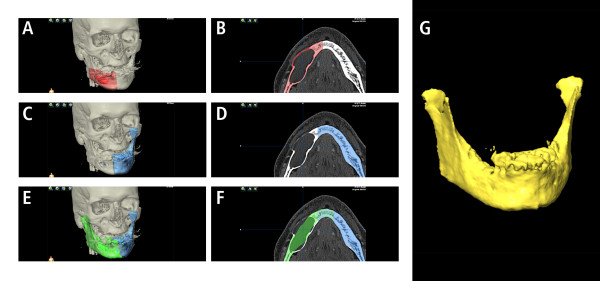
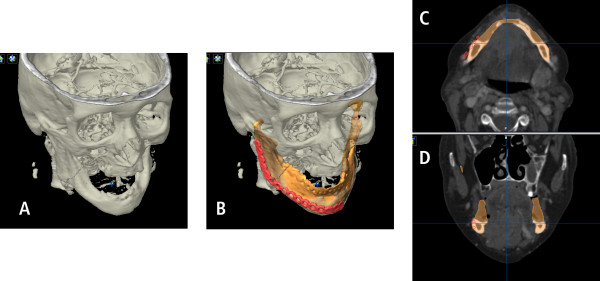
Objectives: Reconstruction of large mandiblular defects following ablative oncologic surgery could be done by using vascularized bone transfer or, more often, primarily with simultaneous or delayed bone grafting, using load bearing reconstruction plates. Bending of these reconstruction plates is typically directed along the outer contour of the original mandible. Simultaneously or in a second operation vascularized or non-vascularized bone is fixed to the reconstruction plate. However, the prosthodontic-driven backward planning to ease bony reconstruction of the mandible in terms of dental rehabilitation using implant-retained overdentures might be an eligible solution. The purpose of this work was to develop, establish and clinically evaluate a novel 3D planning procedure for mandibular reconstruction.
Materials and methods: Three patients with tumors involving the mandible, which included squamous cell carcinoma in the floor of the mouth and keratocystic odontogenic tumor, were treated surgically by hemimandibulectomy.
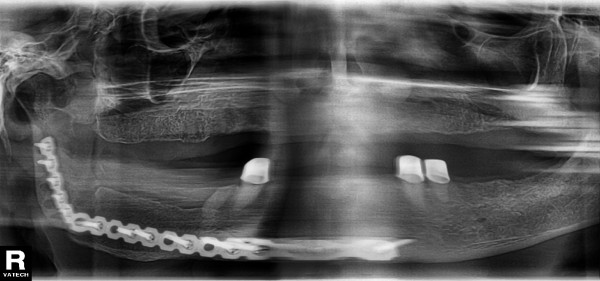
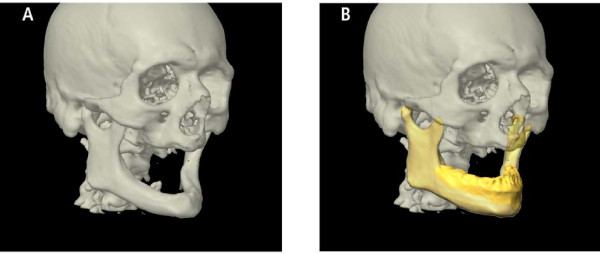
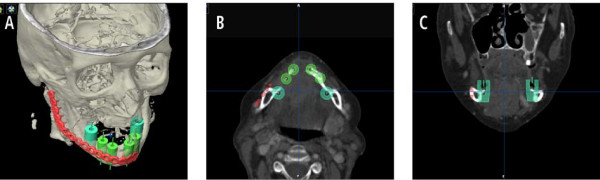
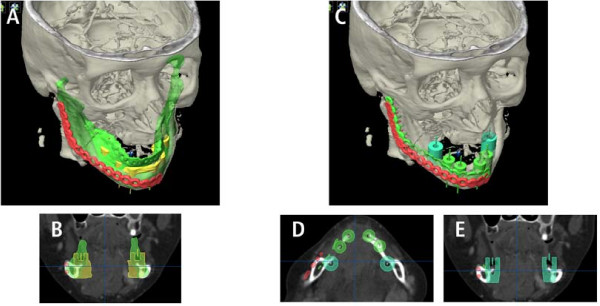
Results: In primary alloplastic mandible reconstruction, shape and size of the reconstruction plate could be predefined and prebent prior to surgery.
Clinical relevance: This study provides modern treatment strategies for mandibular reconstruction.
Figures
References
-
- Mooren RE. et al.Reconstruction of the mandible using preshaped 2.3-mm titanium plates, autogenous cortical bone plates, particulate cancellous bone, and platelet-rich plasma: a retrospective analysis of 20 patients. Journal of oral and maxillofacial surgery: official journal of the American Association of Oral and Maxillofacial Surgeons. 2010;68(10):2459–67. doi: 10.1016/j.joms.2009.12.006. - DOI - PubMed
-
- Schoen PJ. et al.Prosthodontic rehabilitation of oral function in head-neck cancer patients with dental implants placed simultaneously during ablative tumour surgery: an assessment of treatment outcomes and quality of life. International journal of oral and maxillofacial surgery. 2008;37(1):8–16. doi: 10.1016/j.ijom.2007.07.015. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
