

Pharmacokinetics-pharmacodynamics of tigecycline in patients with community-acquired pneumonia
- PMID: 21968360
- PMCID: PMC3256083
- DOI: 10.1128/AAC.00277-10
Pharmacokinetics-pharmacodynamics of tigecycline in patients with community-acquired pneumonia
Abstract
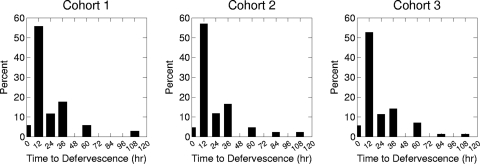
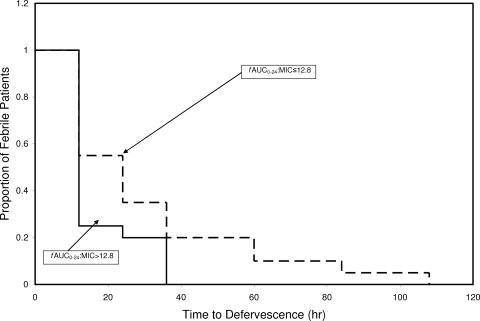
Exposure-response analyses for efficacy and safety were performed for tigecycline-treated patients suffering from community-acquired pneumonia. Data were collected from two randomized, controlled clinical trials in which patients were administered a 100-mg loading dose followed by 50 mg of tigecycline every 12 h. A categorical endpoint, success or failure, 7 to 23 days after the end of therapy (test of cure) and a continuous endpoint, time to fever resolution, were evaluated for exposure-response analyses for efficacy. Nausea/vomiting, diarrhea, headache, and changes in blood urea nitrogen concentration (BUN) and total bilirubin were evaluated for exposure-response analyses for safety. For efficacy, ratios of the free-drug area under the concentration-time curve at 24 h to the MIC of the pathogen (fAUC(0-24):MIC) of ≥12.8 were associated with a faster time to fever resolution; patients with lower drug exposures had a slower time to fever resolution (P = 0.05). For safety, a multivariable logistic regression model demonstrated that a tigecycline AUC above a threshold of 6.87 mg · hr/liter (P = 0.004) and female sex were predictive of the occurrence of nausea and/or vomiting (P = 0.004). Although statistically significant, the linear relationship between tigecycline exposure and maximum change from baseline in total bilirubin is unlikely to be clinically significant.
Figures

Similar articles
-
Pharmacological and patient-specific response determinants in patients with hospital-acquired pneumonia treated with tigecycline.Antimicrob Agents Chemother. 2012 Feb;56(2):1065-72. doi: 10.1128/AAC.01615-10. Epub 2011 Dec 5. Antimicrob Agents Chemother. 2012. PMID: 22143524 Free PMC article. Clinical Trial.
-
Efficacy and safety of tigecycline versus levofloxacin for community-acquired pneumonia.BMC Pulm Med. 2009 Sep 9;9:44. doi: 10.1186/1471-2466-9-44. BMC Pulm Med. 2009. PMID: 19740418 Free PMC article. Clinical Trial.
-
Safety and efficacy of intravenous tigecycline in treatment of community-acquired pneumonia: results from a double-blind randomized phase 3 comparison study with levofloxacin.Diagn Microbiol Infect Dis. 2009 Jan;63(1):52-61. doi: 10.1016/j.diagmicrobio.2008.09.001. Epub 2008 Nov 5. Diagn Microbiol Infect Dis. 2009. PMID: 18990531 Clinical Trial.
-
Tigecycline for the treatment of patients with community-acquired pneumonia requiring hospitalization.Expert Rev Anti Infect Ther. 2009 Oct;7(8):913-23. doi: 10.1586/eri.09.73. Expert Rev Anti Infect Ther. 2009. PMID: 19803699 Review.
-
Tigecycline: in community-acquired pneumonia.Drugs. 2008;68(18):2633-44. doi: 10.2165/0003495-200868180-00008. Drugs. 2008. PMID: 19093704 Review.
Cited by
-
Randomized, Double-Blind, Placebo-Controlled Studies of the Safety and Pharmacokinetics of Single and Multiple Ascending Doses of Eravacycline.Antimicrob Agents Chemother. 2018 Oct 24;62(11):e01174-18. doi: 10.1128/AAC.01174-18. Print 2018 Nov. Antimicrob Agents Chemother. 2018. PMID: 30150464 Free PMC article. Clinical Trial.
-
In Vivo Pharmacodynamic Characterization of a Novel Odilorhabdin Antibiotic, NOSO-502, against Escherichia coli and Klebsiella pneumoniae in a Murine Thigh Infection Model.Antimicrob Agents Chemother. 2018 Aug 27;62(9):e01067-18. doi: 10.1128/AAC.01067-18. Print 2018 Sep. Antimicrob Agents Chemother. 2018. PMID: 29987156 Free PMC article.
-
Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021.Intensive Care Med. 2021 Nov;47(11):1181-1247. doi: 10.1007/s00134-021-06506-y. Epub 2021 Oct 2. Intensive Care Med. 2021. PMID: 34599691 Free PMC article. No abstract available.
-
In Vivo Pharmacodynamic Target Assessment of Eravacycline against Escherichia coli in a Murine Thigh Infection Model.Antimicrob Agents Chemother. 2017 Jun 27;61(7):e00250-17. doi: 10.1128/AAC.00250-17. Print 2017 Jul. Antimicrob Agents Chemother. 2017. PMID: 28416552 Free PMC article.
-
Contemporary Perspective on the Treatment of Acinetobacter baumannii Infections: Insights from the Society of Infectious Diseases Pharmacists.Infect Dis Ther. 2021 Dec;10(4):2177-2202. doi: 10.1007/s40121-021-00541-4. Epub 2021 Oct 14. Infect Dis Ther. 2021. PMID: 34648177 Free PMC article. Review.
References
-
- Ambrose PG. 2008. Use of pharmacokinetics and pharmacodynamics in a failure analysis of community-acquired pneumonia: implications for future clinical trial study design. Clin. Infect. Dis. 47:S225–S231 - PubMed
-
- Carney S, Butcher RA, Dawborn JK, Pattison G. 1974. Minocycline excretion and distribution in relation to renal function in man. Clin. Exp. Pharmacol. Physiol. 1:299–308 - PubMed
-
- Passarell JA, et al. 2005. Pharmacokinetic/pharmacodynamic model for the tolerability of tigecycline in healthy volunteers. 15th Eur. Cong. Clin. Microbiol. Infect. Dis., abstr. P894
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
