

Long-term follow-up of participants with heart failure in the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT)
- PMID: 21969009
- PMCID: PMC3217334
- DOI: 10.1161/CIRCULATIONAHA.110.012575
Long-term follow-up of participants with heart failure in the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT)
Abstract
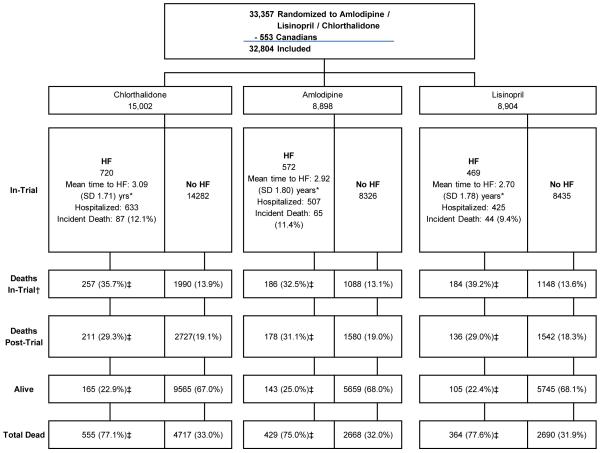
Background: In the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT), a randomized, double-blind, practice-based, active-control, comparative effectiveness trial in high-risk hypertensive participants, risk of new-onset heart failure (HF) was higher in the amlodipine (2.5-10 mg/d) and lisinopril (10-40 mg/d) arms compared with the chlorthalidone (12.5-25 mg/d) arm. Similar to other studies, mortality rates following new-onset HF were very high (≥50% at 5 years), and were similar across randomized treatment arms. After the randomized phase of the trial ended in 2002, outcomes were determined from administrative databases.
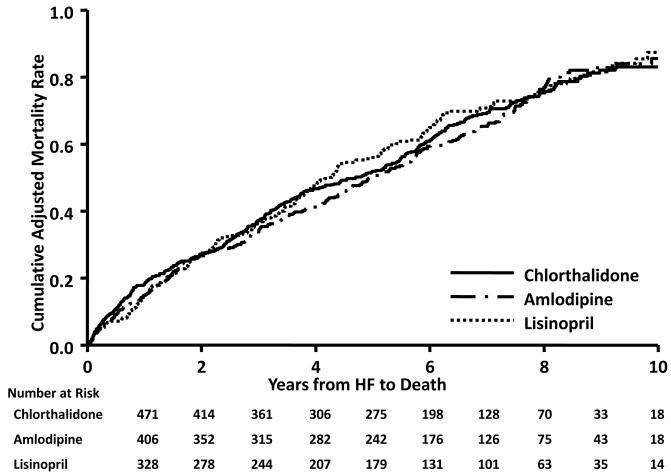
Methods and results: With the use of national databases, posttrial follow-up mortality through 2006 was obtained on participants who developed new-onset HF during the randomized (in-trial) phase of ALLHAT. Mean follow-up for the entire period was 8.9 years. Of 1761 participants with incident HF in-trial, 1348 died. Post-HF all-cause mortality was similar across treatment groups, with adjusted hazard ratios (95% confidence intervals) of 0.95 (0.81-1.12) and 1.05 (0.89-1.25), respectively, for amlodipine and lisinopril compared with chlorthalidone, and 10-year adjusted rates of 86%, 87%, and 83%, respectively. All-cause mortality rates were also similar among those with reduced ejection fractions (84%) and preserved ejection fractions (81%), with no significant differences by randomized treatment arm.
Conclusions: Once HF develops, risk of death is high and consistent across randomized treatment groups. Measures to prevent the development of HF, especially blood pressure control, must be a priority if mortality associated with the development of HF is to be addressed. Clinical Trial Registration- http://www.clinicaltrials.gov. Unique identifier: NCT00000542.
Figures
Comment in
-
Hypertension and heart failure: the ALLHAT imperative.Circulation. 2011 Oct 25;124(17):1803-5. doi: 10.1161/CIRCULATIONAHA.111.059303. Circulation. 2011. PMID: 22025634 No abstract available.
References
-
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, Ford E, Furie K, Go A, Greenlund K, Haase N, Hailpern S, Ho M, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott M, Meigs J, Mozaffarian D, Nichol G, O’Donnell C, Roger V, Rosamond W, Sacco R, Sorlie P, Stafford R, Steinberger J, Thom T, Wasserthiel-Smoller S, Wong N, Wylie-Rosett J, Hong Y, American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:e21–181. - PubMed
-
- Haldeman GA, Croft JB, Giles WH, Rashidee A. Hospitalization of patients with heart failure: National Hospital Discharge Survey, 1985 to 1995. Am Heart J. 1999;137:352–360. - PubMed
-
- Loehr LR, Rosamond WD, Chang PP, Folsom AR, Chambless LE. Heart failure incidence and survival (from the Atherosclerosis Risk in Communities study) Am J Cardiol. 2008;101:1016–1022. - PubMed
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM, Vasan RS. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347:1397–1402. - PubMed
-
- Kostis JB, Davis BR, Cutler J, Grimm RH, Jr, Berge KG, Cohen JD, Lacy CR, Perry HM, Jr, Blaufox MD, Wassertheil-Smoller S, Black HR, Schron E, Berkson DM, Curb JD, Smith WM, McDonald R, Applegate WB. Prevention of heart failure by antihypertensive drug treatment in older persons with isolated systolic hypertension. SHEP Cooperative Research Group. JAMA. 1997;278:212–216. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
