

A prospective evaluation of a protocol for magnetic resonance imaging of patients with implanted cardiac devices
- PMID: 21969340
- PMCID: PMC4337840
- DOI: 10.7326/0003-4819-155-7-201110040-00004
A prospective evaluation of a protocol for magnetic resonance imaging of patients with implanted cardiac devices
Abstract
Background: Magnetic resonance imaging (MRI) is avoided in most patients with implanted cardiac devices because of safety concerns.
Objective: To define the safety of a protocol for MRI at the commonly used magnetic strength of 1.5 T in patients with implanted cardiac devices.
Design: Prospective nonrandomized trial. (ClinicalTrials.gov registration number: NCT01130896) SETTING: One center in the United States (94% of examinations) and one in Israel.
Patients: 438 patients with devices (54% with pacemakers and 46% with defibrillators) who underwent 555 MRI studies.
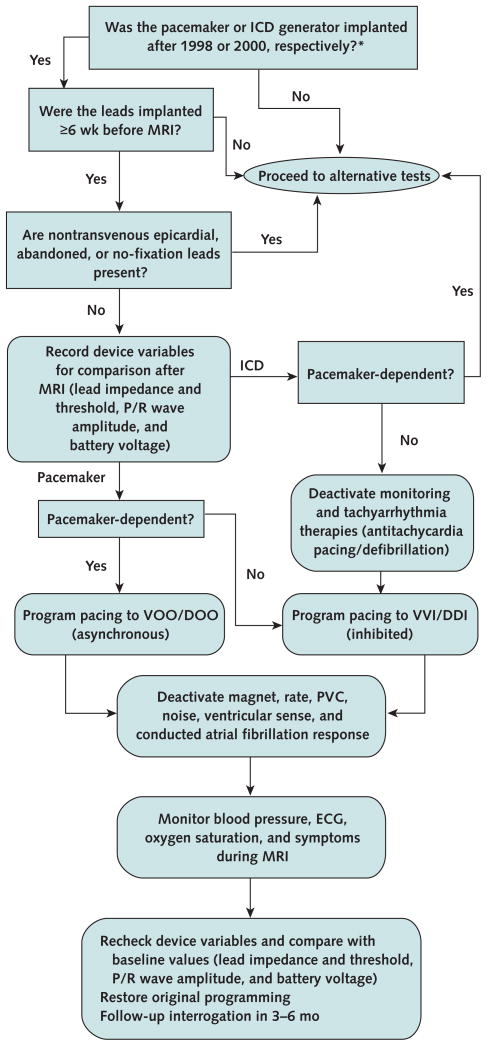
Intervention: Pacing mode was changed to asynchronous for pacemaker-dependent patients and to demand for others. Tachyarrhythmia functions were disabled. Blood pressure, electrocardiography, oximetry, and symptoms were monitored by a nurse with experience in cardiac life support and device programming who had immediate backup from an electrophysiologist.
Measurements: Activation or inhibition of pacing, symptoms, and device variables.
Results: In 3 patients (0.7% [95% CI, 0% to 1.5%]), the device reverted to a transient back-up programming mode without long-term effects. Right ventricular (RV) sensing (median change, 0 mV [interquartile range {IQR}, -0.7 to 0 V]) and atrial and right and left ventricular lead impedances (median change, -2 Ω [IQR, -13 to 0 Ω], -4 Ω [IQR, -16 to 0 Ω], and -11 Ω [IQR, -40 to 0 Ω], respectively) were reduced immediately after MRI. At long-term follow-up (61% of patients), decreased RV sensing (median, 0 mV, [IQR, -1.1 to 0.3 mV]), decreased RV lead impedance (median, -3 Ω, [IQR, -29 to 15 Ω]), increased RV capture threshold (median, 0 V, IQR, [0 to 0.2 Ω]), and decreased battery voltage (median, -0.01 V, IQR, -0.04 to 0 V) were noted. The observed changes did not require device revision or reprogramming.
Limitations: Not all available cardiac devices have been tested. Long-term in-person or telephone follow-up was unavailable in 43 patients (10%), and some data were missing. Those with missing long-term capture threshold data had higher baseline right atrial and right ventricular capture thresholds and were more likely to have undergone thoracic imaging. Defibrillation threshold testing and random assignment to a control group were not performed.
Conclusion: With appropriate precautions, MRI can be done safely in patients with selected cardiac devices. Because changes in device variables and programming may occur, electrophysiologic monitoring during MRI is essential.
Conflict of interest statement
Figures
Comment in
-
Magnetic resonance imaging and cardiac devices: how safe is safe enough?Ann Intern Med. 2011 Oct 4;155(7):470-2. doi: 10.7326/0003-4819-155-7-201110040-00010. Ann Intern Med. 2011. PMID: 21969346 No abstract available.
Summary for patients in
-
Summaries for patients. The safety of magnetic resonance imaging in patients with pacemakers or defibrillators.Ann Intern Med. 2011 Oct 4;155(7):I34. doi: 10.7326/0003-4819-155-7-201110040-00002. Ann Intern Med. 2011. PMID: 21969352 No abstract available.
References
-
- Kalin R, Stanton MS. Current clinical issues for MRI scanning of pacemaker and defibrillator patients. Pacing Clin Electrophysiol. 2005;28:326–8. - PubMed
-
- Levine GN, Gomes AS, Arai AE, Bluemke DA, Flamm SD, Kanal E, et al. American Heart Association Committee on Diagnostic and Interventional Cardiac Catheterization. Safety of magnetic resonance imaging in patients with cardiovascular devices: an American Heart Association scientific statement from the Committee on Diagnostic and Interventional Cardiac Catheterization, Council on Clinical Cardiology, and the Council on Cardiovascular Radiology and Intervention: endorsed by the American College of Cardiology Foundation, the North American Society for Cardiac Imaging, and the Society for Cardiovascular Magnetic Resonance. Circulation. 2007;116:2878–91. - PubMed
-
- Gimbel JR, Johnson D, Levine PA, Wilkoff BL. Safe performance of magnetic resonance imaging on five patients with permanent cardiac pacemakers. Pacing Clin Electrophysiol. 1996;19:913–9. - PubMed
-
- Sommer T, Vahlhaus C, Lauck G, von Smekal A, Reinke M, Hofer U, et al. MR imaging and cardiac pacemakers: in-vitro evaluation and in-vivo studies in 51 patients at 0.5 T. Radiology. 2000;215:869–79. - PubMed
-
- Vahlhaus C, Sommer T, Lewalter T, Schimpf R, Schumacher B, Jung W, et al. Interference with cardiac pacemakers by magnetic resonance imaging: are there irreversible changes at 0. 5 Tesla? Pacing Clin Electrophysiol. 2001;24:489–95. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical