

Cost-effectiveness of second-line antihyperglycemic therapy in patients with type 2 diabetes mellitus inadequately controlled on metformin
- PMID: 21969406
- PMCID: PMC3216433
- DOI: 10.1503/cmaj.110178
Cost-effectiveness of second-line antihyperglycemic therapy in patients with type 2 diabetes mellitus inadequately controlled on metformin
Abstract
Background: Metformin is widely accepted as first-line pharmacotherapy for patients with type 2 diabetes mellitus when glycemic control cannot be achieved by lifestyle interventions alone. However, uncertainty exists regarding the optimal second-line therapy for patients whose diabetes is inadequately controlled by metformin monotherapy. Increased use of newer, more costly agents, along with the rising incidence of type 2 diabetes, carries significant budgetary implications for health care systems. We conducted this analysis to determine the relative costs, benefits and cost-effectiveness of options for second-line treatment of type 2 diabetes.
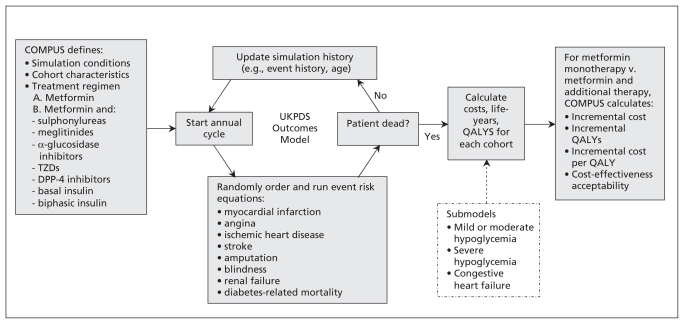
Methods: We used the United Kingdom Prospective Diabetes Study Outcomes Model to forecast diabetes-related complications, quality-adjusted life-years and costs of alternative second-line therapies available in Canada for adults with type 2 diabetes inadequately controlled by metformin. We obtained clinical data from a systematic review and mixed treatment comparison meta-analysis, and we obtained information on costs and utilities from published sources. We performed extensive sensitivity analyses to test the robustness of results to variation in inputs and assumptions.
Results: Sulphonylureas, when added to metformin, were associated with the most favourable cost-effectiveness estimate, with an incremental cost of $12 757 per quality-adjusted life-year gained, relative to continued metformin monotherapy. Treatment with other agents, including thiazolidinediones and dipeptidyl peptidase-4 inhibitors, had unfavourable cost-effectiveness estimates compared with sulphonylureas. These results were robust to extensive sensitivity analyses.
Interpretation: For most patients with type 2 diabetes that is inadequately controlled with metformin monotherapy, the addition of a sulphonylurea represents the most cost-effective second-line therapy.
Figures

References
-
- Canadian Diabetes Association Canadian Diabetes Association 2008 clinical practice guidelines for the prevention and management of diabetes in Canada. Can J Diabetes 2008;32 Suppl 1: i-S201 Available: www.diabetes.ca/files/cpg2008/cpg-2008.pdf (accessed 2011 July 4).
-
- Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycaemia in type 2 diabetes mellitus: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2009; 52:17–30 - PubMed
-
- UK Prospective Diabetes Study Group UK Prospective Diabetes Study 16. Overview of 6 years’ therapy of type II diabetes: a progressive disease. Diabetes 1995;44:1249–58 - PubMed
-
- Current utilization of second- and third-line therapies in patients with type 2 diabetes. CADTH Optimal Therapy Report 4(3). Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2010. Available: www.cadth.ca/media/pdf/C1110-CU-Report-2nd-3rd-Line-Agents-final-e.pdf (accessed 2011 July 4).
-
- Quick reference guide. Type 2 diabetes: the management of type 2 diabetes. London (UK): National Institute for Health and Clinical Excellence; 2009. [updated 2010]. Available: www.nice.org.uk/nicemedia/pdf/CG87QuickRefGuide.pdf (accessed 2011 July 4).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical