

Prediction of early death after induction therapy for newly diagnosed acute myeloid leukemia with pretreatment risk scores: a novel paradigm for treatment assignment
- PMID: 21969499
- PMCID: PMC3221524
- DOI: 10.1200/JCO.2011.35.7525
Prediction of early death after induction therapy for newly diagnosed acute myeloid leukemia with pretreatment risk scores: a novel paradigm for treatment assignment
Abstract
Purpose: Outcome in acute myeloid leukemia (AML) worsens with age, at least in part because of higher treatment-related mortality (TRM) in older patients. Eligibility for intensive AML treatment protocols is therefore typically based on age as the implied principal predictor of TRM, although other health- and disease-related factors modulate this age effect.
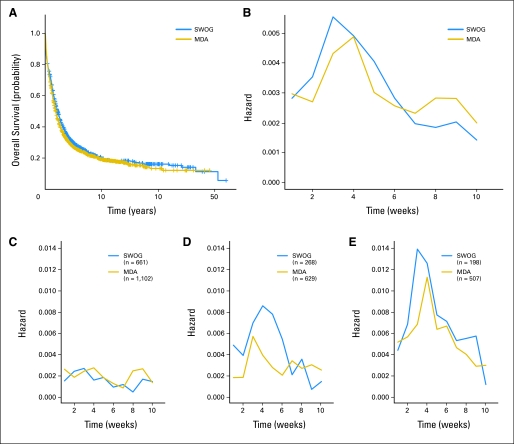
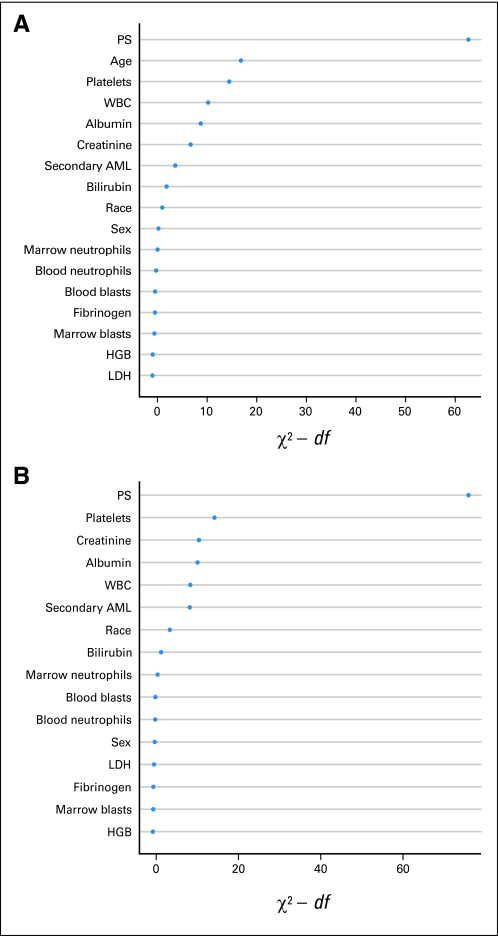
Patients and methods: We empirically defined TRM using estimated weekly hazard rates in 3,365 adults of all ages administered intensive chemotherapy for newly diagnosed AML. We used the area under the receiver operator characteristic curve (AUC) to quantify the relative effects of age and other covariates on TRM in a subset of 2,238 patients. In this approach, an AUC of 1.0 denotes perfect prediction, whereas an AUC of 0.5 is analogous to a coin flip.
Results: Regardless of age, risk of death declined once 4 weeks had elapsed from treatment start, suggesting that patients who die during this time comprise a qualitatively distinct group. Performance status (PS) and age were the most important individual predictors of TRM (AUCs of 0.75 and 0.65, respectively). However, multicomponent models were significantly more accurate in predicting TRM (AUC of 0.83) than PS or age alone. Elimination of age from such multicomponent models only minimally affected their predictive accuracy (AUC of 0.82).
Conclusion: These data suggest that age is primarily a surrogate for other covariates, which themselves add significantly to predictive accuracy, thus challenging the wisdom of using age as primary or sole basis for assignment of intensive, curative intent treatment in AML.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Prediction of early death in acute myeloid leukemia.J Clin Oncol. 2012 Feb 1;30(4):462-3; author reply 463-4. doi: 10.1200/JCO.2011.40.0580. Epub 2011 Dec 19. J Clin Oncol. 2012. PMID: 22184399 No abstract available.
References
-
- Altekruse SF, Kosary CL, Krapcho M, et al. Bethesda, MD: National Cancer Institute; 2010. Childhood Cancer by the ICCC: SEER Cancer Statistics Review, 1975-2007. http://seer.cancer.gov/csr/1975_2007.
-
- Altekruse SF, Kosary CL, Krapcho M, et al. Bethesda, MD: National Cancer Institute; 2010. Leukemia: SEER Cancer Statistics Review, 1975-2007. http://seer.cancer.gov/csr/1975_2007.
-
- Estey E, Smith TL, Keating MJ, et al. Prediction of survival during induction therapy in patients with newly diagnosed acute myeloblastic leukemia. Leukemia. 1989;3:257–263. - PubMed
-
- Giles FJ, Borthakur G, Ravandi F, et al. The haematopoietic cell transplantation comorbidity index score is predictive of early death and survival in patients over 60 years of age receiving induction therapy for acute myeloid leukaemia. Br J Haematol. 2007;136:624–627. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
