

Quantitative CT improves outcome prediction in acute traumatic brain injury
- PMID: 21970562
- PMCID: PMC3303103
- DOI: 10.1089/neu.2011.2008
Quantitative CT improves outcome prediction in acute traumatic brain injury
Abstract
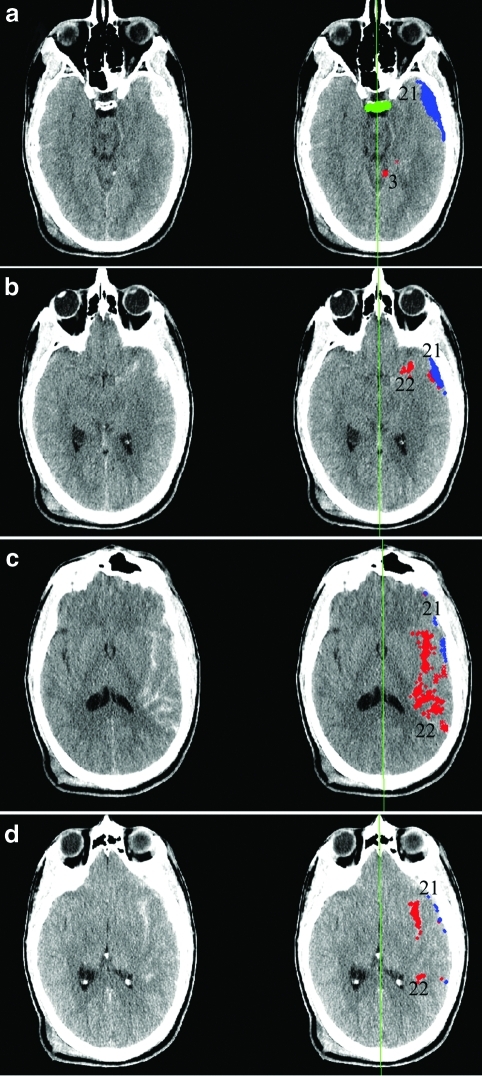
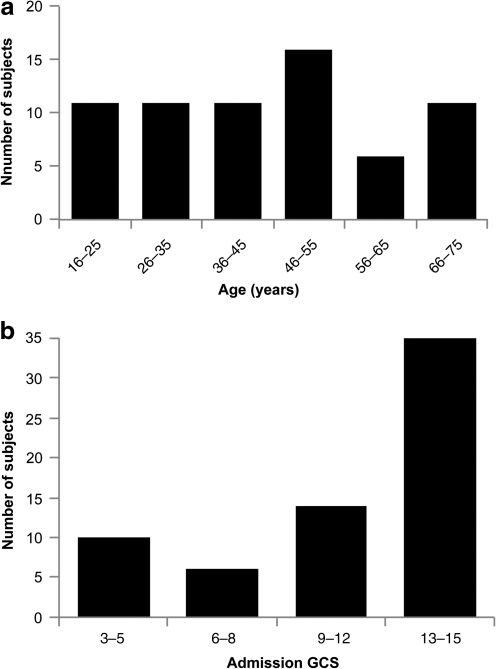
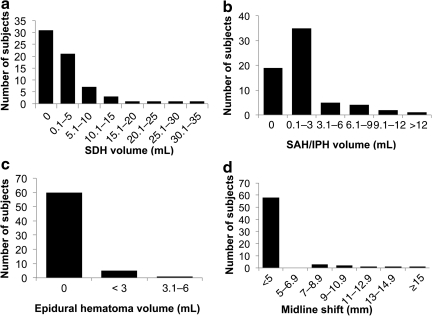
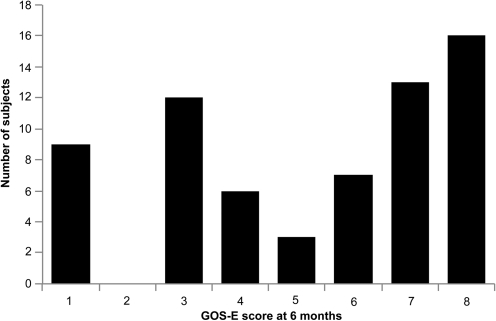
The admission noncontrast head computed tomography (CT) scan has been demonstrated to be one of several key early clinical and imaging features in the challenging problem of prediction of long-term outcome after acute traumatic brain injury (TBI). In this study, we employ two novel approaches to the problem of imaging classification and outcome prediction in acute TBI. First, we employ the novel technique of quantitative CT (qCT) image analysis to provide more objective, reproducible measures of the abnormal features of the admission head CT in acute TBI. We show that the incorporation of quantitative, rather than qualitative, CT features results in a significant improvement in prediction of the 6-month Extended Glasgow Outcome Scale (GOS-E) score over a wide spectrum of injury severity. Second, we employ principal components analysis (PCA) to demonstrate the interdependence of certain predictive variables. Relatively few prior studies of outcome prediction in acute TBI have used a multivariate approach that explicitly takes into account the potential covariance among clinical and CT predictive variables. We demonstrate that several predictors, including midline shift, cistern effacement, subdural hematoma volume, and Glasgow Coma Scale (GCS) score are related to one another. Rather than being independent features, their importance may be related to their status as surrogate measures of a more fundamental underlying clinical feature, such as the severity of intracranial mass effect. We believe that objective computational tools and data-driven analytical methods hold great promise for neurotrauma research, and may ultimately have a role in image analysis for clinical care.
Figures

References
-
- Chestnut R.M. Ghajar J. Maas A.I. Marion D.W. Servadei F. Teasdale G.M. Unterberg A. von Holst H. Walters B.C. Management and prognosis of severe traumatic brain injury. Part 2: Early indicators of prognosis in severe traumatic brain injury. J. Neurotrauma. 2000;17:557–627.
-
- Chieregato A. Fainardi E. Morselli-Labate A.M. Antonelli V. Compagnone C. Targa L. Kraus J. Servadei F. Factors associated with neurological outcome and lesion progression in traumatic subarachnoid hemorrhage patients. Neurosurgery. 2005;56:671–680. - PubMed
-
- Eisenberg H.M. Gary H.E., Jr. Aldrich E.F. Saydjari C. Turner B. Foulkes M.A. Jane J.A. Marmarou A. Marshall L.F. Young H.F. Initial CT findings in 753 patients with severe head injury: A report from the NIH Traumatic Coma Data Bank. J. Neurosurg. 1990;73:688–698. - PubMed
-
- Hukkelhoven C.W. Steyerberg E.W. Habbema J.D. Farace E. Marmarou A. Murray G.D. Marshall L.F. Maas A.I. Predicting outcome after traumatic brain injury: Development and validation of a prognostic score based on admission characteristics. J. Neurotrauma. 2005;22:1025–1039. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
