

A short tapered stem reduces intraoperative complications in primary total hip arthroplasty
- PMID: 21971877
- PMCID: PMC3254753
- DOI: 10.1007/s11999-011-2068-7
A short tapered stem reduces intraoperative complications in primary total hip arthroplasty
Abstract
Background: While short-stem design is not a new concept, interest has surged with increasing utilization of less invasive techniques. Short stems are easier to insert through small incisions. Reliable long-term results including functional improvement, pain relief, and implant survival have been reported with standard tapered stems, but will a short taper perform as well?
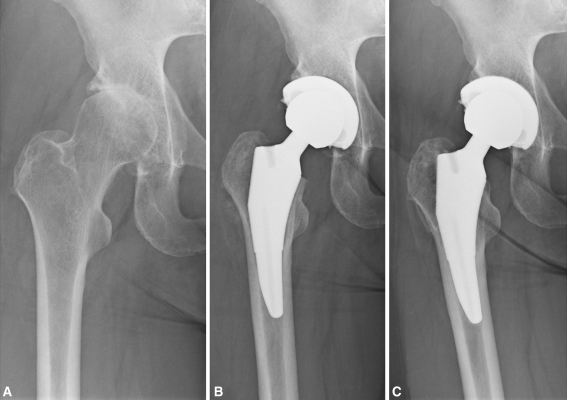
Questions/purposes: We compared short, flat-wedge, tapered, broach-only femoral stems to standard-length, double-tapered, ream and broach femoral stems in terms of intraoperative complications, short-term survivorship, and pain and function scores.
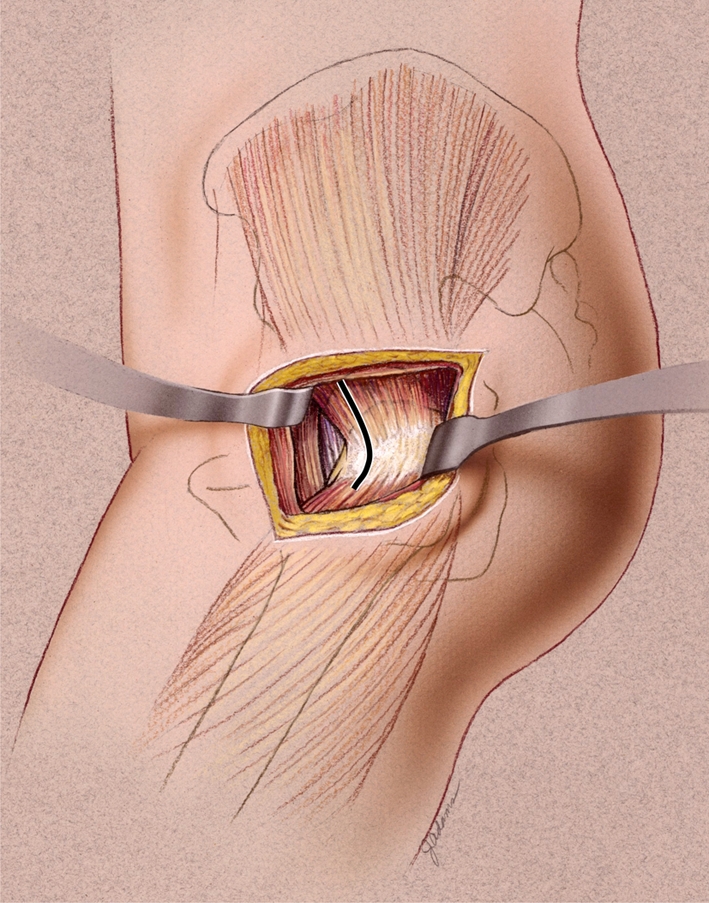
Patients and methods: We retrospectively reviewed the records of 606 patients who had 658 THAs using a less invasive direct lateral approach from January 2006 to March 2008. Three hundred sixty patients (389 hips) had standard-length stems and 246 (269 hips) had short stems. Age averaged 63 years, and body mass index averaged 30.7 kg/m(2). We recorded complications and pain and function scores and computed short-term survival. Minimum followup was 0.8 months (mean, 29.2 months; range, 0.8-62.2 months).
Results: We observed a higher rate of intraoperative complications with the standard-length stems (3.1%; three trochanteric avulsions, nine femoral fractures) compared with the shorter stems (0.4%; one femoral fracture) and managed all complications with application of one or more cerclage cables. There were no differences in implant survival, Harris hip score, and Lower Extremity Activity Scale score between groups.
Conclusions: Fewer intraoperative complications occurred with the short stems, attesting to the easier insertion of these devices. While longer followup is required, our early results suggest shortened stems can be used with low complication rates and do not compromise the survival and functional outcome of cementless THA.
Level of evidence: Level III, therapeutic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures



References
-
- Andrew TA, Flanagan JP, Gerundini M, Bombelli R. The isoelastic, noncemented total hip arthroplasty: preliminary experience with 400 cases. Clin Orthop Relat Res. 1986;206:127–138. - PubMed
-
- Au MK. Isoelastic total hip replacement: clinical evaluation of prosthetic isoelasticity. J Formos Med Assoc. 1994;93:497–502. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
