

Effects of intravenous immunoglobulin therapy in Japanese patients with polymyositis and dermatomyositis resistant to corticosteroids: a randomized double-blind placebo-controlled trial
- PMID: 21971943
- PMCID: PMC3375426
- DOI: 10.1007/s10165-011-0534-4
Effects of intravenous immunoglobulin therapy in Japanese patients with polymyositis and dermatomyositis resistant to corticosteroids: a randomized double-blind placebo-controlled trial
Abstract
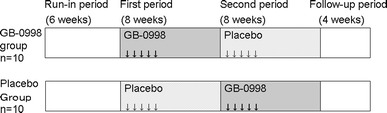
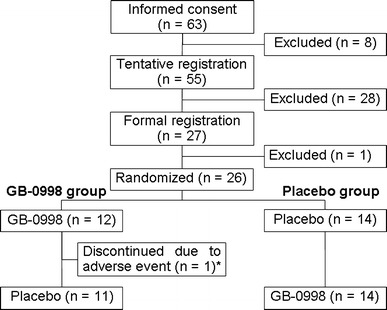
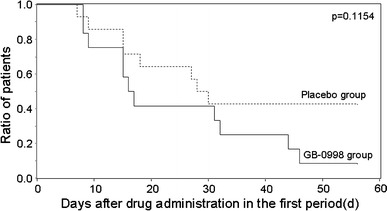
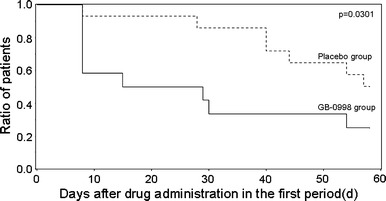
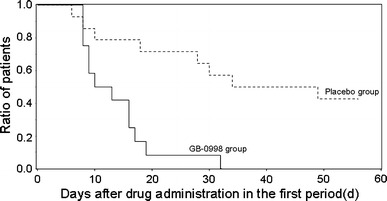
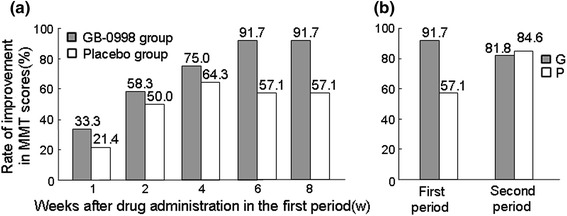
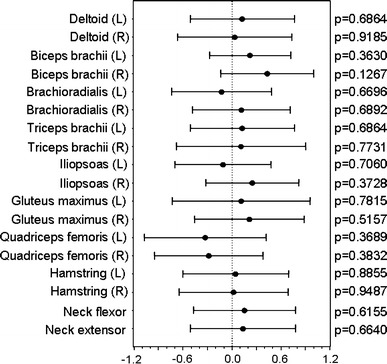
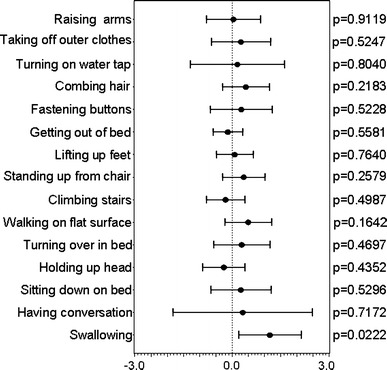
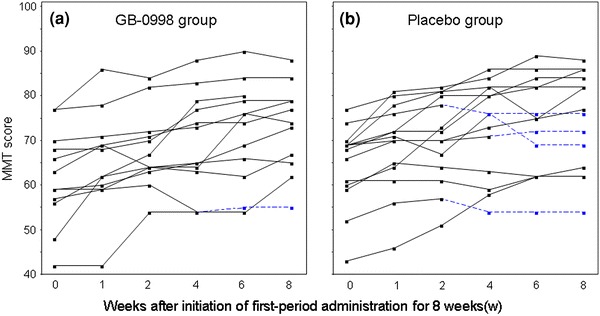
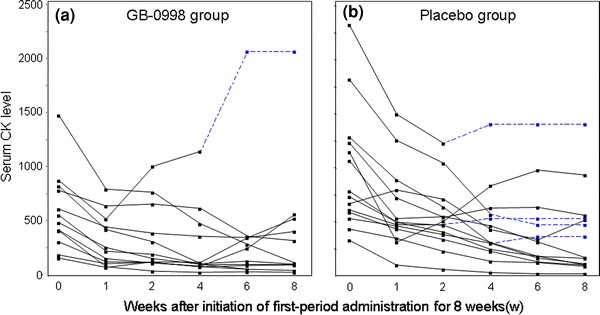
High-dose intravenous immunoglobulin (IVIG) therapy has been effective in treating various autoimmune and systemic inflammatory diseases. Here, we assessed the efficacy and safety of IVIG therapy with polyethylene glycol-treated human IgG (drug code GB-0998) for patients with corticosteroid-refractory polymyositis (PM) and dermatomyositis (DM) by means of a randomized, double-blind, placebo-controlled study. We randomly assigned 26 subjects (16 PM and 10 DM) to receive either GB-0998 or placebo. Intragroup comparison in the GB-0998 group showed statistically significant improvements due to GB-0998 administration in the primary endpoint (manual muscle test score) and secondary endpoints (serum creatine kinase level and activities of daily living score). However, significant improvements were also found in the placebo group, and comparison of the GB-0998 group with the placebo group did not show any significant difference between the groups. We discuss possible reasons for the absence of a clear intergroup difference in efficacy. Nineteen adverse drug reactions were observed in 11 of 26 subjects (42.3%), of which 2 events (decreased muscle strength and increased serum creatine kinase) were assessed as serious; however, they are previously known events. These results indicate that GB-0998 can be safely used with the same precautions as other current IVIG therapy.
Figures
References
-
- Bradley WG. Polymyositis. Br J Hosp Med. 1977;17:351–355. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
