

Determination of cranio-spinal canal compliance distribution by MRI: Methodology and early application in idiopathic intracranial hypertension
- PMID: 21972076
- PMCID: PMC3221868
- DOI: 10.1002/jmri.22799
Determination of cranio-spinal canal compliance distribution by MRI: Methodology and early application in idiopathic intracranial hypertension
Abstract
Purpose: To develop a method for derivation of the cranial-spinal compliance distribution, assess its reliability, and apply to obese female patients with a diagnosis of idiopathic intracranial hypertension (IIH).
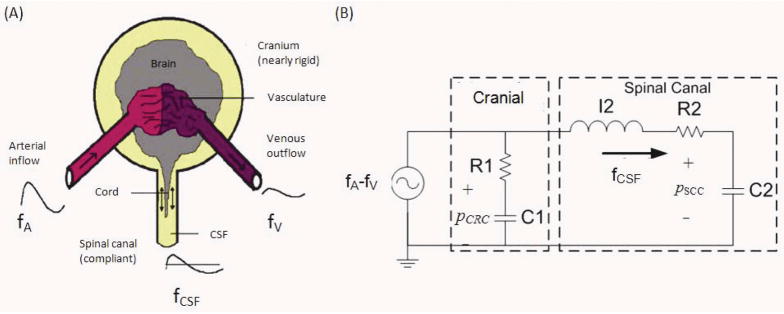
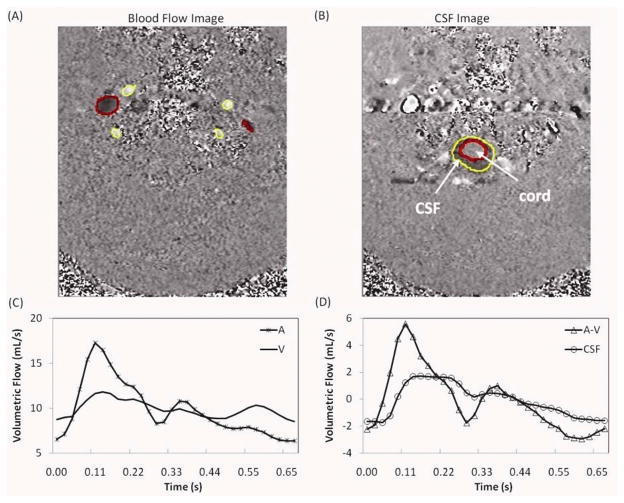
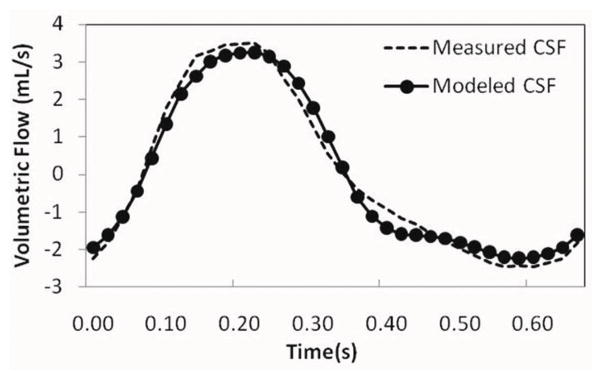
Materials and methods: Phase contrast-based measurements of blood and cerebrospinal fluid (CSF) flows to, from, and between the cranial and spinal canal compartments were used with lumped-parameter modeling to estimate systolic volume and pressure changes from which cranial and spinal compliance indices are obtained. The proposed MRI indices are analogous to pressure volume indices (PVI) currently being measured invasively with infusion-based techniques. The consistency of the proposed method was assessed using MRI data from seven aged healthy subjects. Measurement reproducibility was assessed using five repeated MR scans from one subject. The method was then applied to compare spinal canal compliance contribution in seven IIH patients and six matched healthy controls.
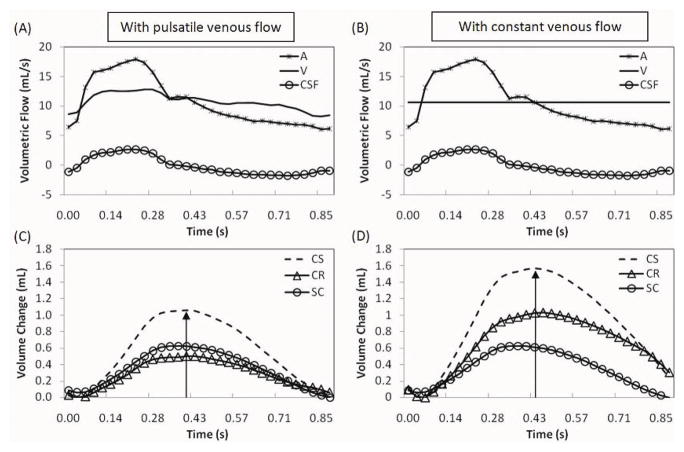
Results: In the healthy subjects, as expected, spinal canal contribution was consistently larger than the cranial contribution (average value of 69%). Measurement variability was 8%. In IIH, the spinal canal contribution is significantly smaller than normal controls (60 versus 78%, P < 0.03).
Conclusion: An MRI-based method for derivation of compliance indices analogous to PVI has been implemented and applied to healthy subjects. The application of the method to obese IIH patients suggests a spinal canal involvement in the pathophysiology of IIH.
Copyright © 2011 Wiley Periodicals, Inc.
Figures
References
-
- Löfgren J, von Essen C, Zwetnow N. The pressure-volume curve of the cerebrospinal fluid space in dogs. Acta Neurol Scand. 1973;49:557–574. - PubMed
-
- Marmarou A, Shulman K, LaMorgese J. Compartmental analysis of compliance and outflow resistance of the cerebrospinal fluid system. J Neurosurg. 1975;43:523–534. - PubMed
-
- Magnaes B. Clinical studies of cranial and spinal compliance and the craniospinal flow of cerebrospinal fluid. Br J Neurosurg. 1989;3:659–668. - PubMed
-
- Alperin N, Lee S, Sivaramakrishnan A, Hushek S. Quantifying the effect of posture on intracranial physiology in humans by MRI flow studies. J Magn Reson Imaging. 2005;22:591–596. - PubMed
-
- Maset AL, Marmarou A, Ward JD, et al. Pressure-volume index in head injury. J Neurosurg. 1987;67:832–840. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
