

Creating and evaluating a data-driven curriculum for central venous catheter placement
- PMID: 21976088
- PMCID: PMC2951779
- DOI: 10.4300/JGME-D-10-00007.1
Creating and evaluating a data-driven curriculum for central venous catheter placement
Abstract
Background: Central venous catheter placement is a common procedure with a high incidence of error. Other fields requiring high reliability have used Failure Mode and Effects Analysis (FMEA) to prioritize quality and safety improvement efforts.
Objective: To use FMEA in the development of a formal, standardized curriculum for central venous catheter training.
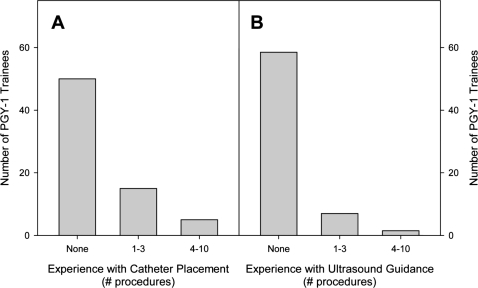
Methods: We surveyed interns regarding their prior experience with central venous catheter placement. A multidisciplinary team used FMEA to identify high-priority failure modes and to develop online and hands-on training modules to decrease the frequency, diminish the severity, and improve the early detection of these failure modes. We required new interns to complete the modules and tracked their progress using multiple assessments.
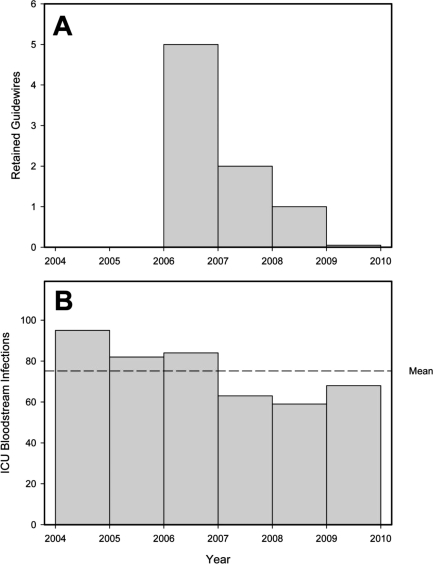
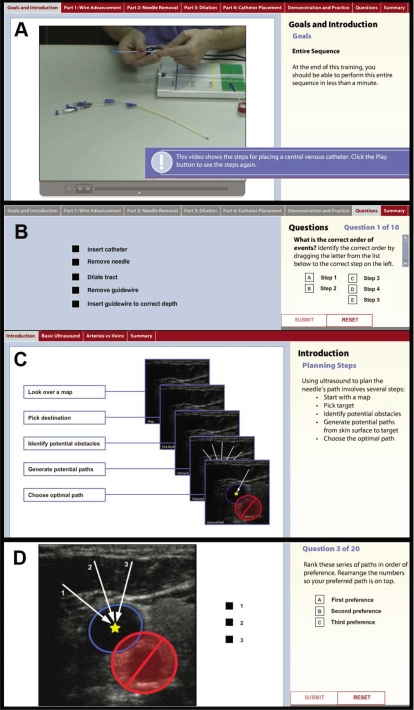
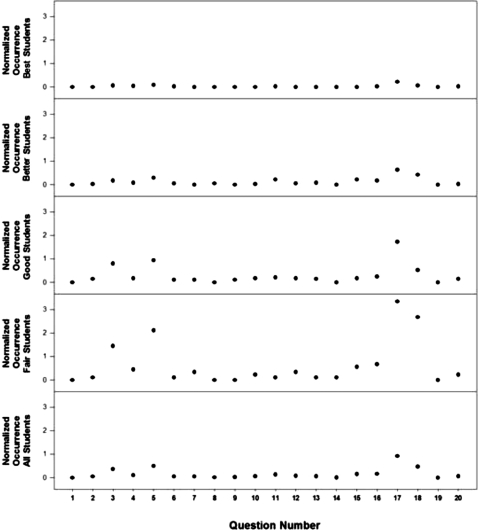
Results: Survey results showed new interns had little prior experience with central venous catheter placement. Using FMEA, we created a curriculum that focused on planning and execution skills and identified 3 priority topics: (1) retained guidewires, which led to training on handling catheters and guidewires; (2) improved needle access, which prompted the development of an ultrasound training module; and (3) catheter-associated bloodstream infections, which were addressed through training on maximum sterile barriers. Each module included assessments that measured progress toward recognition and avoidance of common failure modes. Since introducing this curriculum, the number of retained guidewires has fallen more than 4-fold. Rates of catheter-associated infections have not yet declined, and it will take time before ultrasound training will have a measurable effect.
Conclusion: The FMEA provided a process for curriculum development. Precise definitions of failure modes for retained guidewires facilitated development of a curriculum that contributed to a dramatic decrease in the frequency of this complication. Although infections and access complications have not yet declined, failure mode identification, curriculum development, and monitored implementation show substantial promise for improving patient safety during placement of central venous catheters.
Figures
References
-
- Merrer J., De Jonghe B., Golliot F., et al. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. JAMA. 2001;286(6):700–707. - PubMed
-
- Sznajder J. I., Zveibil F. R., Bitterman H., Weiner P., Bursztein S. Central vein catheterization. Failure and complication rates by three percutaneous approaches. Arch Intern Med. 1986;146(2):259–261. - PubMed
-
- Mansfield P. F., Hohn D. C., Fornage B. D., Gregurich M. A., Ota D. M. Complications and failures of subclavian-vein catheterization. N Engl J Med. 1994;331(26):1735–1738. - PubMed
-
- Martin C., Eon B., Auffray J. P., Saux P., Gouin F. Axillary or internal jugular central venous catheterization. Crit Care Med. 1990;18(4):400–402. - PubMed
-
- Sridhar S., Duncan J. R. Strategies for choosing process improvement projects. J Vasc Interv Radiol. 2008;19(4):471–477. - PubMed
LinkOut - more resources
Full Text Sources