

Murine models of vaginal trichomonad infections
- PMID: 21976570
- PMCID: PMC3183775
- DOI: 10.4269/ajtmh.2011.11-0123
Murine models of vaginal trichomonad infections
Abstract
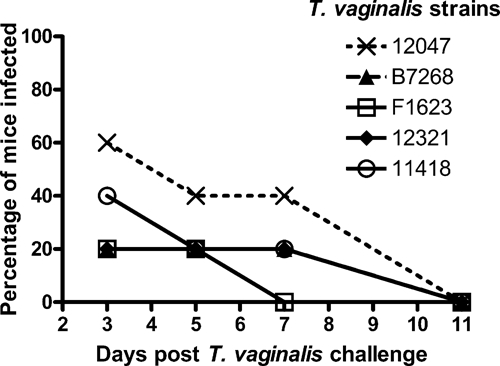
Trichomonas vaginalis and Tritrichomonas foetus cause common sexually transmitted infections in humans and cattle, respectively. Mouse models of trichomoniasis are important for pathogenic and therapeutic studies. Here, we compared murine genital infections with T. vaginalis and T. foetus. Persistent vaginal infection with T. foetus was established with 100 parasites but T. vaginalis infection required doses of 10(6), perhaps because of greater susceptibility to killing by mouse vaginal polymorphonuclear leukocytes. Infection with T. vaginalis persisted longest after combined treatment of mice with estrogen and dexamethasone, whereas infection was only short-lived when mice were given estrogen or dexamethasone alone, co-infected with Lactobacillus acidophilus, and/or pretreated with antibiotics. Infection rates were similar with metronidazole-resistant (MR) and metronidazole-sensitive (MS) T. vaginalis. High dose but not low dose metronidazole treatment controlled infection with MS better than MR T. vaginalis. These murine models will be valuable for investigating the pathogenesis and treatment of trichomoniasis.
Figures





References
-
- Nanda N, Michel R, Kurdgelashvili G, Wendel K. Trichomoniasis and its treatment. Expert Rev Anti Infect Ther. 2006;4:125–135. - PubMed
-
- Parsonson IM, Clark BL, Dufty JH. Early pathogenesis and pathology of Tritrichomonas foetus infection in virgin heifers. J Comp Pathol. 1976;86:59–66. - PubMed
-
- Rhyan JC, Stackhouse LL, Quinn WJ. Fetal and placental lesions in bovine abortion due to Tritrichomonas foetus. Vet Pathol. 1988;25:350–355. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
