

Aggregate evaluable organ dysfunction predicts in-hospital mortality from sepsis in Uganda
- PMID: 21976575
- PMCID: PMC3183780
- DOI: 10.4269/ajtmh.2011.10-0692
Aggregate evaluable organ dysfunction predicts in-hospital mortality from sepsis in Uganda
Abstract
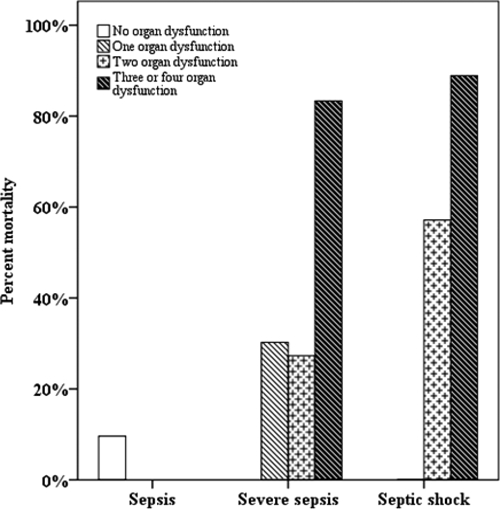
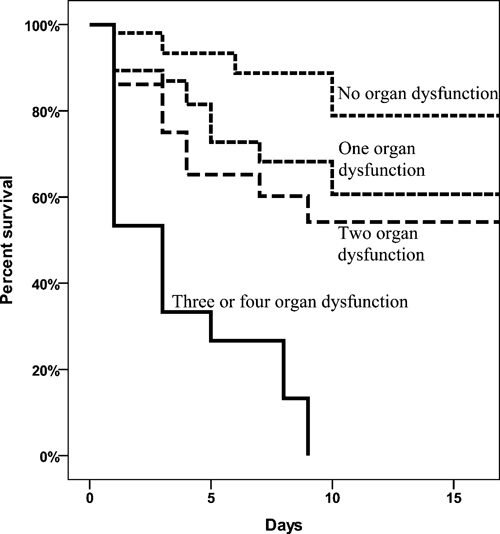
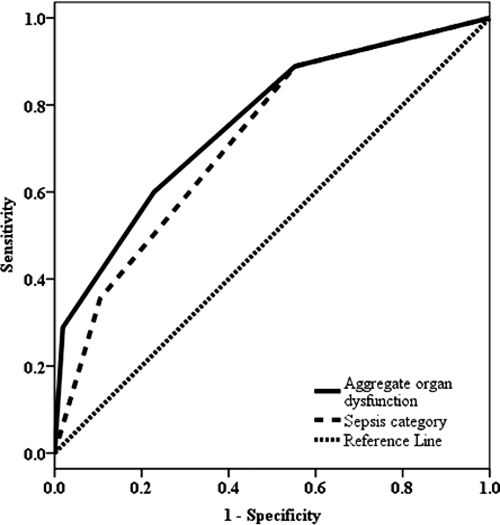
We evaluated the association between severity of sepsis and in-hospital mortality in 150 patients with non-surgical sepsis at a regional referral hospital in Uganda. In-hospital mortality occurred in 5 of 52 (9.6%) patients with sepsis, 24 of 71 (33.8%) patients with severe sepsis, and 16 of 27 (59.3%) patients with septic shock. In the multivariate analysis, the identification of severe sepsis (adjusted hazard ratio [AHR] = 2.9, 95% confidence interval [CI] = 1.0-8.2, P = 0.04), septic shock (AHR = 5.7, 95% CI = 1.6-20.3, P = 0.007), and dysfunction of three or more organs (AHR = 2.9, 95% CI = 1.1-7.3, P = 0.03) increased the risk of in-hospital mortality. Adding aggregate organ dysfunction to the multivariate equation that included the sepsis category statistically significantly improved the model, but the opposite did not. Predictors of mortality were easily measurable and could be used to risk stratify critically ill patients in resource-constrained settings.
Figures
References
-
- World Health Organization . The Global Burden of Disease (2004 Update) Geneva, Switzerland: World Health Organization; 2008.
-
- Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31:1250–1256. - PubMed
-
- Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med. 1995;23:1638–1652. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
