

Immunodiagnosis of tuberculosis: a dynamic view of biomarker discovery
- PMID: 21976609
- PMCID: PMC3194832
- DOI: 10.1128/CMR.00014-11
Immunodiagnosis of tuberculosis: a dynamic view of biomarker discovery
Abstract
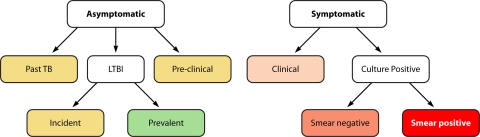
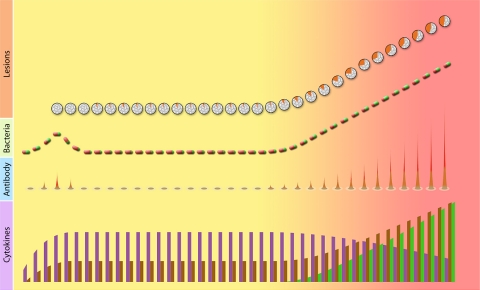
Infection with Mycobacterium tuberculosis causes a variety of clinical conditions ranging from life-long asymptomatic infection to overt disease with increasingly severe tissue damage and a heavy bacillary burden. Immune biomarkers should follow the evolution of infection and disease because the host immune response is at the core of protection against disease and tissue damage in M. tuberculosis infection. Moreover, levels of immune markers are often affected by the antigen load. We review how the clinical spectrum of M. tuberculosis infection correlates with the evolution of granulomatous lesions and how granuloma structural changes are reflected in the peripheral circulation. We also discuss how antigen-specific, peripheral immune responses change during infection and how these changes are associated with the physiology of the tubercle bacillus. We propose that a dynamic approach to immune biomarker research should overcome the challenges of identifying those asymptomatic and symptomatic stages of infection that require antituberculosis treatment. Implementation of such a view requires longitudinal studies and a systems immunology approach leading to multianalyte assays.
Figures
References
-
- Abebe F., Holm-Hansen C., Wiker H. G., Bjune G. 2007. Progress in serodiagnosis of Mycobacterium tuberculosis infection. Scand. J. Immunol. 66:176–191 - PubMed
-
- American Thoracic Society 2000. Diagnostic standards and classification of tuberculosis in adults and children. Am. J. Respir. Crit. Care Med. 161:1376–1395 - PubMed
-
- American Thoracic Society 2000. Targeted tuberculin testing and treatment of latent tuberculosis infection. MMWR Recommend. Rep. 49:1–51 - PubMed
-
- Andersen P., Doherty T. M., Pai M., Weldingh K. 2007. The prognosis of latent tuberculosis: can disease be predicted? Trends Mol. Med. 13:175–182 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
