

The bronchoalveolar lavage pattern in radiation pneumonitis secondary to radiotherapy for breast cancer
- PMID: 21977166
- PMCID: PMC3152839
The bronchoalveolar lavage pattern in radiation pneumonitis secondary to radiotherapy for breast cancer
Abstract
Background and purpose: Radiotherapy in breast cancer patients is limited by lung tissue tolerance. Two complications involving the lung are known: radiation pneumonitis (RP) and radiation fibrosis. The aim of the study was to evaluate the pattern of bronchoalveolar lavage (BAL) in patients with RP after radiotherapy for breast cancer in symptomatic and asymptomatic patients.
Material and methods: Sixty-five female patients (mean age 58.3 yrs) with RP after radiotherapy for breast cancer were included in the study. The majority of patients had previous breast surgery (mastectomy or lumpectomy and axillary dissection) and received doses of radiations of 45-50Gy. All patients had adjuvant chemotherapy with cyclophosphamide, 5-fluorouracil, and epirubicin or methotrexate.
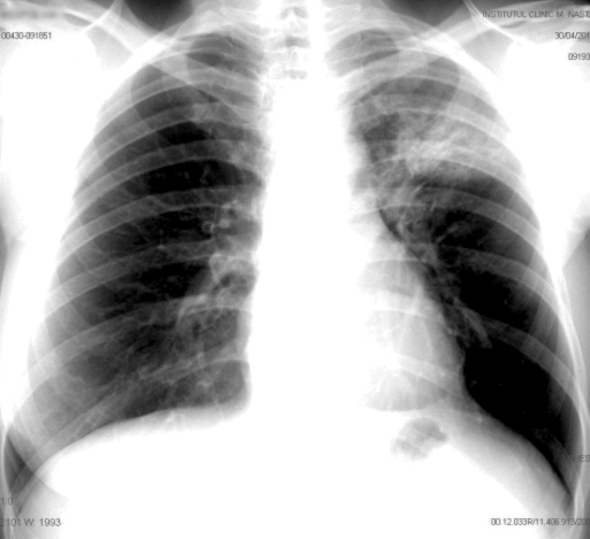
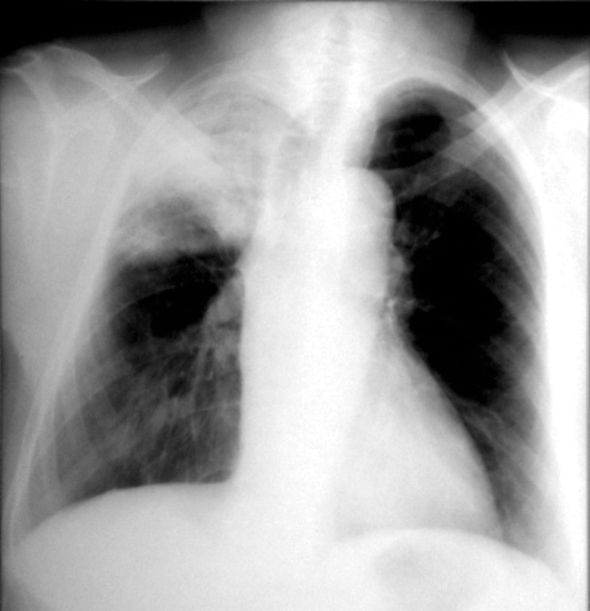
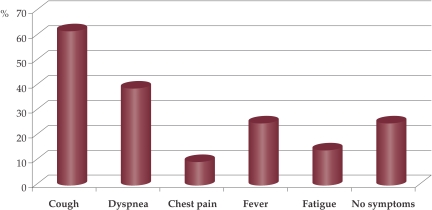
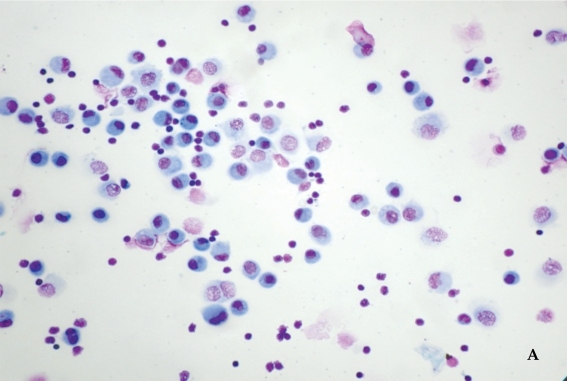
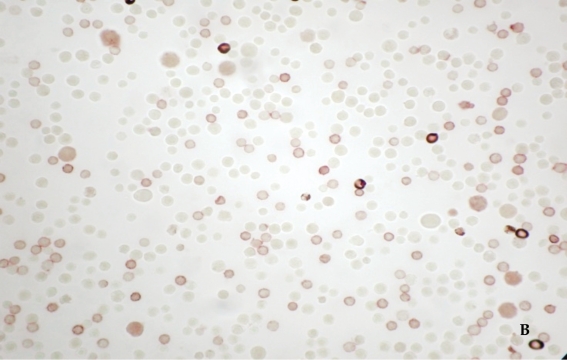
Results: All patients had an infiltrate or consolidation on chest radiography confined to the upper lobe of the irradiated lung, as marker of RP. Based on the presence or absence of symptoms, we divided the patients in 2 groups: 49 patients (75.4%) with symptomatic RP (fever, cough, dyspnea, chest pain and fatigue) and 16 patients (24.6%) without any symptom. Symptomatic RP patients had a BAL with significant increase in total cells (18.0±12.2 x10(6) cells•100mL-1) when compared to BAL in asymptomatic patients (11.9±6.2 x10(6) cells•100mL-1), p=0.01. Lymphocytosis in BAL was significantly increased in symptomatic group, compared with asymptomatic one (35.4±18.7% vs. 26.1±14.3%, p=0.045), with predominance of T lymphocytes (CD3). It was also a predominance of CD4 lymphocytes in all patients, but the CD4/CD8 ratio was inside normal range in the majority of cases. Five patients had clinical features of bronchiolitis obliterans organizing pneumonia (BOOP) secondary to irradiation with increased percentages of lymphocytes, neutrophils, eosinophils, and mast cells in BAL and one patient without history of atopic disease had a percentage of 40% eosinophils. Only a mild reduction in diffusing capacity for carbon monoxide was seen in both groups on pulmonary function tests. The lung volumes were normal in all patients.
Conclusions: Lymphocytic alveolitis was the marker of radiation pneumonitis in all patients. The degree of the inflammatory reaction of the lungs was correlated with the presence of symptoms. The lymphocytic alveolitis consisted mainly of T lymphocytes, with a predominance of CD4 subset in both groups, but the CD4/CD8 ratio remained mostly into normal range.
Keywords: breast cancer; bronchoalveolar lavage; lymphocytosis; radiation pneumonitis.
Conflict of interest statement
Figures
References
-
- Bate D, Guttmann RJ. Changes in lung and pleura following 2-million volt therapy for carcinoma of the breast. Radiology. 1957;69:372–382. - PubMed
-
- Gross NJ. Pulmonary effects of radiation therapy. Ann.Intern.Med. 1977;86:81–92. - PubMed
-
- Davis SD, Yankelevitz DF, Henschke CI. Radiation effects on the lung: clinical features, pathology, and imaging findings. AJR Am.J.Roentgenol. 1992;159:1157–1164. - PubMed
-
- Madani I, De Ruyck K K, Goeminne H, et al. Predicting risk of radiation-induced lung injury. J.Thorac.Oncol. 2007;2:864–874. - PubMed
-
- Scherer E E, Streffer C, Trott KR. Radiopathology of Organs and Tissues. Berlin/Heidelberg: Springer-Verlag. 1991
LinkOut - more resources
Full Text Sources
Research Materials