

Systemic inflammation and early atheroma formation: are they related?
- PMID: 21977173
- PMCID: PMC3152836
Systemic inflammation and early atheroma formation: are they related?
Abstract
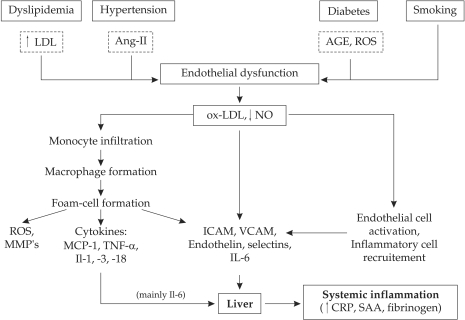
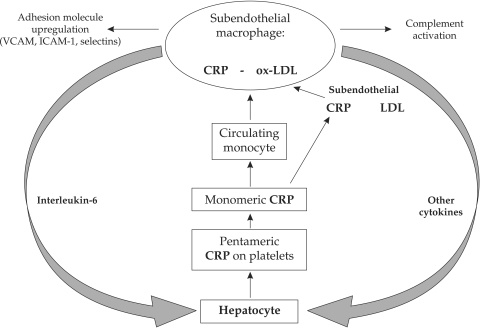
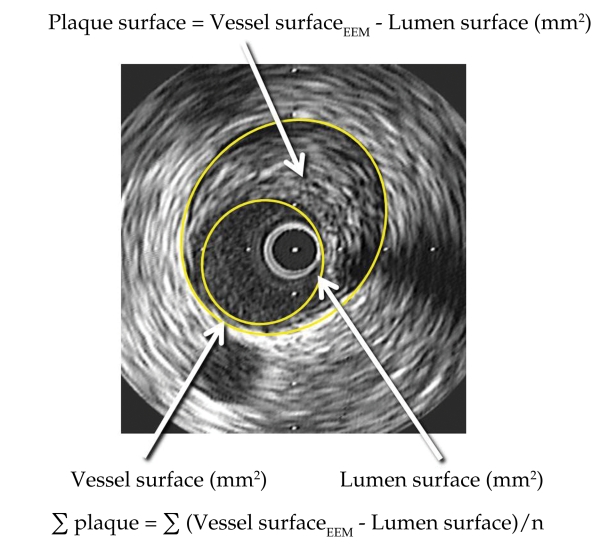
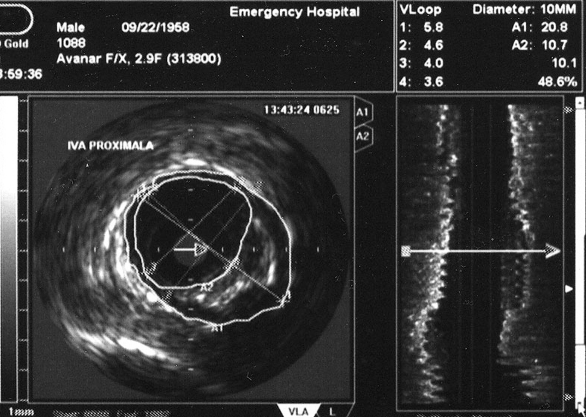
Atherosclerosis is a chronic inflammatory disease started by endothelial injury and defined by arterial wall load with free and esterified cholesterol, followed by subintimal focal recruitment of circulating monocytes and T-lymphocytes that heals by fibrosis and calcification. Inflammation plays a crucial role in atherogenesis either by local cellular mechanisms or humoral consequences easily measurable in plasma. In most cases inflammation and endothelial dysfunction are triggered by cardiovascular risk factors: hypercholesterolemia, hypertension, smoking or diabetes. In other cases inflammation precedes atherosclerotic changes that occur in autoimmune diseases, as systemic lupus erythematosus and rheumatoid arthritis. In these diseases atherogenesis is mostly independent from conventional risk factors. Irrespective of its cause systemic inflammation is correlated with cardiovascular events, but currently there are controversial results regarding inflammatory markers and early atherosclerotic process. We designed a study to identify if the amplitude of inflammation expressed by multiple serum markers is correlated with the severity of the atherosclerotic process measured by coronary atheroma volume and carotid intima-media thickness. The selected inflammatory markers are associated with different pathogenic steps in atherogenesis: acute phase reactants (C-reactive protein); pro-inflammatory cytokines (TNF-alpha, interleukin-6 and -18); endothelium activation markers (soluble VCAM-1, ICAM-1); and specific factors (anticardiolipinic antibodies). We aim to enrol the two different patient subsets with early atherosclerosis: one with conventional risk factors and one with autoimmune diseases without traditional risk factors, in whom inflammation is part of the systemic disease progression.
Keywords: early atheroma formation; systemic inflammation.
Conflict of interest statement
Figures

References
-
- Ross R. Atherosclerosis: an inflammatory disease. N Engl J Med. 1999;340:115–126. - PubMed
-
- Kinlay S, Egido J. Inflammatory biomarkers in stable atherosclerosis. Am J Cardiol. 2006;98(Suppl):2P–8P. - PubMed
-
- Smith S, Anderson J, Cannon R, et al. DC/AHA Workshop on Markers of Inflammation and Cardiovascular Disease Application to Clinical and Public Health Practice Report From the Clinical Practice Discussion Group. Circulation. 2004;110:e550–e553. - PubMed
-
- Ridker P, Cook N. Clinical usefulness of very high and very low levels of C-reactive protein across the full range of Framingham risk scores. Circulation. 2004;109:1955–1959. - PubMed
-
- Ray K, Cannon C, Ganz P. Beyond lipid lowering: what have we learned about the benefits of statins from the acute coronary syndromes trials? Am J Cardiol. 2006;98(Suppl):18P–25P. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous