

Rates of detection of mood and anxiety disorders in primary care: a descriptive, cross-sectional study
- PMID: 21977354
- PMCID: PMC3184591
- DOI: 10.4088/PCC.10m01013
Rates of detection of mood and anxiety disorders in primary care: a descriptive, cross-sectional study
Abstract
Objective: To determine the incidence of major depressive disorder, bipolar disorder, panic disorder, social anxiety disorder, and generalized anxiety disorder and to assess their detection rates in the Canadian primary care setting.
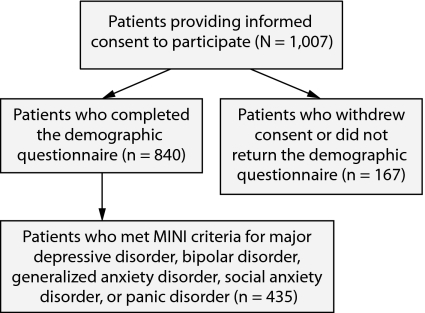
Method: The descriptive, cross-sectional study was conducted in 7 primary care clinics in 3 Canadian provinces, Ontario, British Columbia, and Nova Scotia, from December 6, 2005, to May 5, 2006. Patients in clinic waiting rooms who consented to participate in the study were administered the Mini International Neuropsychiatric Interview (MINI) (N = 840). These patients' medical charts were then reviewed for evidence of previous diagnosis of a mood or anxiety disorder. Misdiagnosis was defined as cases for which a diagnosis was reached on the MINI but not in the patient's chart.
Results: Of the 840 primary care patients assessed, 27.2%, 11.4%, 12.6%, 31.2%, and 16.5% of patients met criteria for major depressive disorder, bipolar disorder, panic disorder, generalized anxiety disorder, and social anxiety disorder, respectively. Misdiagnosis rates reached 65.9% for major depressive disorder, 92.7% for bipolar disorder, 85.8% for panic disorder, 71.0% for generalized anxiety disorder, and 97.8% for social anxiety disorder.
Conclusions: With high prevalence rates and poor detection, there is an obvious need to enhance diagnostic screening in the primary care setting.
Figures
References
-
- Stephens T, Joubert N. The economic burden of mental health problems in Canada. Chronic Dis Can. 2001;22(1):18–23. - PubMed
-
- Statistics Canada. The daily Canadian community health survey: mental health and well-being (Canada Catalogue no. 11-001-XIE) http://www.statcan.ca/Daily/English/030903/d030903.pdf. Accessed October 19, 2006.
-
- Greenberg PE, Sisitsky T, Kessler RC, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry. 1999;60(7):427–435. - PubMed
-
- Weiller E, Bisserbe JC, Boyer P, et al. Social phobia in general health care: an unrecognised undertreated disabling disorder. Br J Psychiatry. 1996;168(2):169–174. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous