

Risk of injury associated with attention-deficit/hyperactivity disorder in adults enrolled in employer-sponsored health plans: a retrospective analysis
- PMID: 21977357
- PMCID: PMC3184594
- DOI: 10.4088/PCC.10m01031
Risk of injury associated with attention-deficit/hyperactivity disorder in adults enrolled in employer-sponsored health plans: a retrospective analysis
Abstract
Objective: Attention-deficit/hyperactivity disorder (ADHD) is linked to an increased risk of injury in children. This retrospective analysis evaluated the risk and type of injury associated with ADHD in adults.
Method: Data were taken from the MarketScan databases, which provide details of health care claims and productivity data for individuals and their dependents with access to employer-sponsored health plans. Adults (aged 18-64 years) with ≥ 2 ADHD-related diagnostic claims (using ICD-9-CM codes) between 2002 and 2007 and evidence of ADHD treatment in 2006 (n = 31,752) were matched to controls without ADHD (1:3; n = 95,256) or individuals with a depression diagnosis (using ICD-9-CM codes; 1:1; n = 29,965). Injury claims were compared between cohorts, and multivariate analyses controlled for differences that remained after matching.
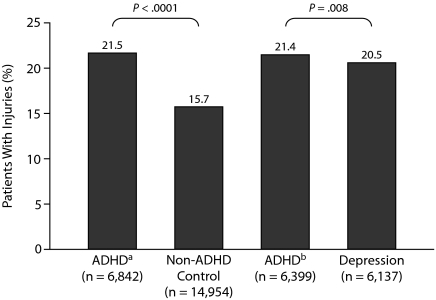
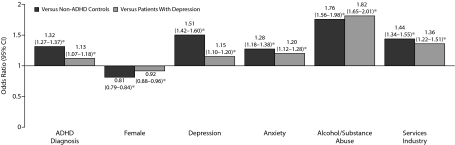
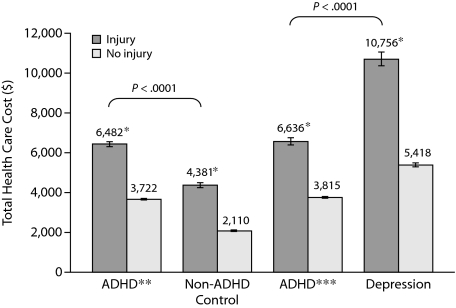
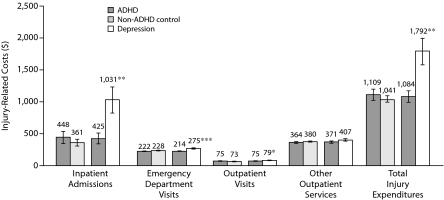
Results: Injury claims were more common in individuals with ADHD than in non-ADHD controls (21.5% vs 15.7%; P< .0001) or individuals with depression (21.4% vs 20.5%; P= .008). Multivariate analyses indicated that the relative risk of injury claims was higher in individuals with ADHD than in the non-ADHD control (odds ratio [OR] = 1.32; 95% CI, 1.27-1.37; P< .01) and depression (OR = 1.13; 95% CI, 1.07-1.18; P< .01) groups. Injury claims increased total direct health care expenditure; total expenditures for ADHD patients with injuries were $6,482 compared with $3,722 for ADHD patients without injuries (P < .0001). Comparison of injury-related costs were similar between ADHD patients and non-ADHD controls ($1,109 vs $1,041, respectively), but higher for depression patients than for ADHD patients ($1,792 vs $1,084; P < .01). Injury claim was also associated with increased short-term disability expenditures, as ADHD patients with injury incurred higher mean cost than those without injury ($1,303 vs $620; P = .0001), but lower than those with injury in the depression cohort (vs $2,152; P = .0099)
Conclusions: Adults with ADHD were more likely to incur injury claims than non-ADHD controls or adults with depression in this sample selected on the basis of claims data rather than clinical referrals. Most injuries were relatively minor; however, individuals with injuries incurred higher total direct health care costs than those without injuries. Furthermore, the ratio of indirect costs due to workplace absence to direct health care costs was higher for adults with ADHD than for adults with depression, demonstrating not only the impact of ADHD in the workplace, but also the importance of accounting for productivity data in calculating the true economic burden of ADHD in adults.
Figures
References
-
- Hammerness P, Surman C, Miller K. Update on adult attention-deficit/hyperactivity disorder. Curr Neurol Neurosci Rep. 2008;8(6):484–489. - PubMed
-
- National Institute for Health and Clinical Excellence. Attention deficit hyperactivity disorder: diagnosis and management of ADHD in children, young people and adults. Clinical guideline 72. National Institute for Health and Clinical Excellence. http://www.nice.org.uk/nicemedia/pdf/ADHDFullGuideline.pdf. Accessed February 24, 2011.
-
- Biederman J, Wilens TE, Spencer TJ, et al. Diagnosis and treatment of adults with attention-deficit/hyperactivity disorder. CNS Spectr. 2007;12(suppl 6):1–15.
-
- Bloom B, Cohen RA, Freeman G. Summary Health Statistics for US Children: National Health Interview Survey, 2007. Vital Health Stat 10. 2009;239(239):1–80. - PubMed
LinkOut - more resources
Full Text Sources