

New pathophysiological concepts underlying pathogenesis of pigment gallstones
- PMID: 21978438
- PMCID: PMC3311771
- DOI: 10.1016/j.clinre.2011.08.010
New pathophysiological concepts underlying pathogenesis of pigment gallstones
Abstract
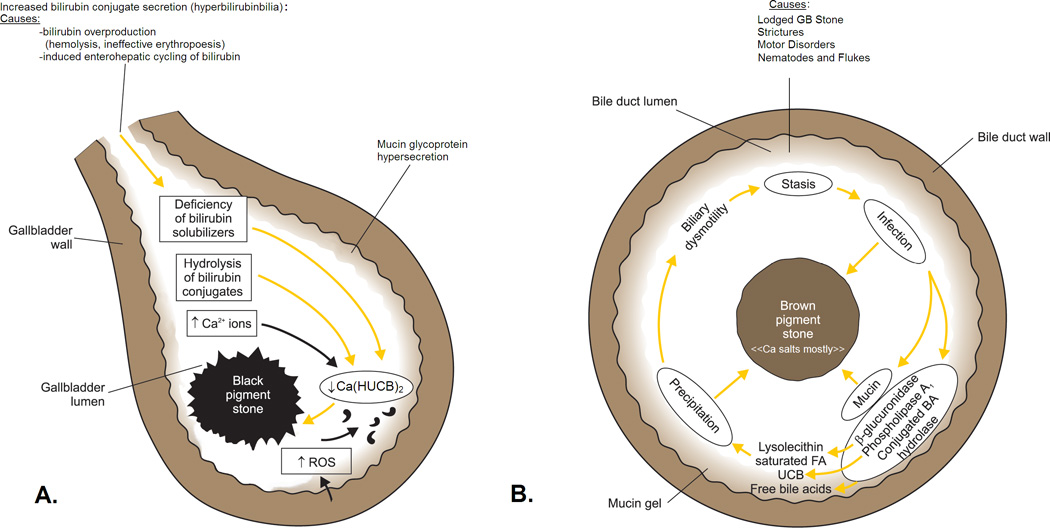
Pigment gallstones, which are much less frequent than cholesterol stones, are classified descriptively as "black" or "brown". They are composed mostly of calcium hydrogen bilirubinate, Ca(HUCB)(2), which is polymerized and oxidized in "black" stones but remains unpolymerized in "brown" stones. Black stones form in sterile gallbladder bile but brown stones form secondary to stasis and anaerobic bacterial infection in any part of the biliary tree, including the gallbladder. Other calcium salts coprecipitate in both stone types; crystalline calcium phosphate and/or carbonate in the case of "black" stones and amorphous calcium salts of long chain saturated fatty acids ("soaps") in the case of "brown" stones. Cholesterol is present in variable proportions in "brown" more than "black" stones and in the latter, the bile sterol may be totally absent. The "scaffolding" of both stone types is a mixed mucin glycoprotein matrix secreted by epithelial cells lining the biliary tree. The critical pathophysiological prerequisite for "black" stone formation is "hyperbilirubinbilia" (biliary hypersecretion of bilirubin conjugates). It is due principally to hemolysis, ineffective erythropoiesis, or pathologic enterohepatic cycling of unconjugated bilirubin. Endogenous biliary β-glucuronidase hydrolysis of bilirubin conjugates in gallbladder bile provides HUCB(-) molecules that precipitate as insoluble salts with ionized Ca. Putatively, reactive oxygen species secreted by an inflamed gallbladder mucosa are responsible for transforming the initial soft yellow precipitates into hard black [Ca(HUCB)(2)](n) polymers. Despite "brown" gallstones being soft and amenable to mechanical removal, chronic anaerobic infection of the biliary tree is often markedly resistant to eradication.
Copyright © 2011 Elsevier Masson SAS. All rights reserved.
Figures
Comment in
-
Role of parietal (gallbladder mucosa) factors in the formation of black pigment gallstones.Clin Res Hepatol Gastroenterol. 2012 Jun;36(3):e50-1; author reply e52-3. doi: 10.1016/j.clinre.2012.02.001. Epub 2012 Apr 30. Clin Res Hepatol Gastroenterol. 2012. PMID: 22551643 No abstract available.
References
-
- Cahalane MJ, Neubrand MW, Carey MC. Physical-chemical pathogenesis of pigment gallstones. Semin Liver Dis. 1988;8:317–328. - PubMed
-
- Suzuki N, Nakamura Y, Kobayashi N, Sato T. On metal elements in pure pigment gallstones. Tohoku J Exp Med. 1975;116:233–240. - PubMed
-
- Tsunoda K, Shirai Y, Wakai T, Yokoyama N, Akazawa K, Hatakeyama K. Increased risk of cholelithiasis after esophagectomy. J Hepatobiliary Pancreat Surg. 2004;11:319–323. - PubMed
-
- Strauss KA, Robinson DL, Vreman HJ, Puffenberger EG, Hart G, Morton DH. Management of hyperbilirubinemia and prevention of kernicterus in 20 patients with Crigler-Najjar disease. Eur J Pediatr. 2006;165:306–319. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
