

Craniocervical arterial dissection in children: diagnosis and treatment
- PMID: 21979145
- PMCID: PMC3297486
- DOI: 10.1007/s11940-011-0149-2
Craniocervical arterial dissection in children: diagnosis and treatment
Abstract
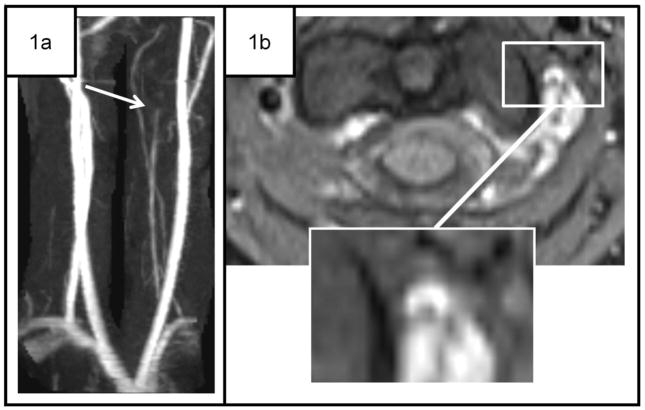
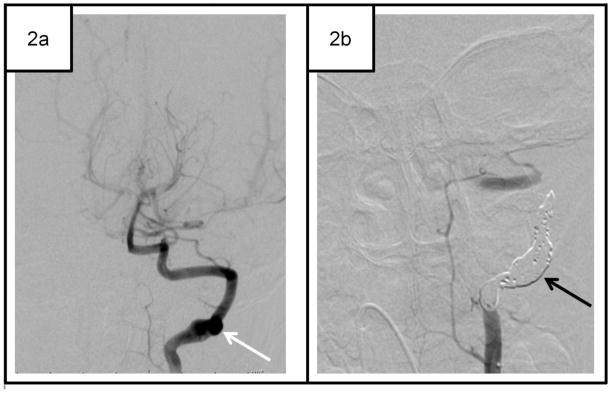
Diagnosis of craniocervical arterial dissection (CCAD) in children begins with a careful history and physical in a child with a transient ischemic attack (TIA) or arterial ischemic stroke (AIS). The extent of radiologic evaluation for suspected CCAD is based upon careful consideration of the risks associated with the best imaging techniques, weighed against the benefits of enhanced vascular imaging with better diagnostic sensitivity. Although conventional angiography (CA) and CT angiography (CTA) have a higher sensitivity than magnetic resonance angiography (MRA), they are accompanied by risks: for CA, femoral hematoma, femoral arterial pseudoaneurysm, recurrent AIS, and radiation exposure; for CTA, radiation. For children (non-neonates) with suspected CCAD, MRI with MRA is recommended as the first-line imaging study. MRI usually includes diffusion-weighted, FLAIR, and T1 images of the brain, and T1 or T2 fat-saturation axial imaging through the neck. MRA should include 3D time-of-flight MRA of the head and neck (from the aortic arch through the circle of Willis). Contrast-enhanced MRA should be highly considered in neck imaging. If MRI/MRA is equivocal, CCAD is strongly suspected but not detected on MRI/MRA (especially in the posterior circulation), or the child has recurrent events, additional imaging of the craniocervical vasculature is likely warranted. Individual clinical circumstances warrant careful, case-by-case consideration. Treatment of CCAD in children is challenging and differs for intracranial and extracranial dissections. In extracranial CCAD, we most commonly use anticoagulation for 6 weeks to 6 months in patients with TIA or AIS. Typically, unfractionated heparin is used in the acutely ill patient at heightened risk for bleeding (because of its short half-life), whereas low-molecular-weight heparin (LMWH) or warfarin are reserved for the stable patient. If the history is suspicious for dissection (head and neck trauma, recent cervical chiropractic manipulation, recent car accident, or neck pain), we consider treatment for dissection even with normal MRI/MRA. For patients with CCAD with a stroke size greater than one third to one half of the middle cerebral artery territory (or other bleeding risk factors) and extracranial CCAD, in whom there is concern about heightened risk for hemorrhagic conversion, we commonly use aspirin therapy during the acute phase. Regardless of their treatment in the initial weeks to months, we subsequently treat all patients with aspirin for 1 year after their event, and sometimes longer if they have other risk factors. Interventional techniques, such as extracranial cerebral arterial stent placement or selective occlusion, are understudied in children. Interventional techniques are typically reserved for patients who fail aggressive medical management and have recurrent TIA or AIS. The diagnosis and treatment of intracranial dissection is extraordinarily challenging in children, in whom inflammatory intracranial arteriopathies are common. When intracranial arteriopathy is clearly associated with dissection, the clinician should look for the presence of subarachnoid hemorrhage and/or dissecting aneurysm. Treatment decisions should be made by a multidisciplinary pediatric stroke team, given the lack of data in this area. Intracranial cerebral artery stent placement carries high risk and is not recommended for intracranial CCAD in children. Most importantly, we educate all children with CCAD and their parents about the paucity of evidence in the treatment of this disease, the risks of enhanced imaging techniques such as CTA or CA, and the challenges involved in weighing the risks of aggressive therapies and interventions against the costs of unclear diagnosis and potentially ineffective treatments. We also educate our patients with CCAD about the signs and symptoms of recurrence and the importance of emergent evaluation.
Conflict of interest statement
No potential conflicts of interest relevant to this article were reported.
Figures
Similar articles
-
Vesicoureteral Reflux.2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 33085409 Free Books & Documents.
-
Outcome of extracranial cervicocephalic arterial dissections: a follow-up study.Neurol Res. 2002 Jun;24(4):395-8. doi: 10.1179/016164102101200087. Neurol Res. 2002. PMID: 12069289
-
Shoulder Arthrogram.2023 Apr 3. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Apr 3. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 35593869 Free Books & Documents.
-
Peripheral Arterial Disease – Diagnosis and Treatment: A Systematic Review [Internet].Stockholm: Swedish Council on Health Technology Assessment (SBU); 2008 Nov. SBU Yellow Report No. 187. Stockholm: Swedish Council on Health Technology Assessment (SBU); 2008 Nov. SBU Yellow Report No. 187. PMID: 28876730 Free Books & Documents. Review.
-
Craniocervical Artery Dissections: A Concise Review for Clinicians.Mayo Clin Proc. 2022 Apr;97(4):777-783. doi: 10.1016/j.mayocp.2022.02.007. Mayo Clin Proc. 2022. PMID: 35379423 Review.
Cited by
-
Cost and Utility of Routine Contrast-Enhanced Neck MRA in a Pediatric MRI Stroke Evaluation Protocol.AJNR Am J Neuroradiol. 2019 Dec;40(12):2143-2145. doi: 10.3174/ajnr.A6315. Epub 2019 Nov 14. AJNR Am J Neuroradiol. 2019. PMID: 31727745 Free PMC article.
-
Atypical Presentation of Traumatic Pediatric Carotid Artery Dissection: A Case Report.Clin Pract Cases Emerg Med. 2022 Aug;6(3):229-231. doi: 10.5811/cpcem.2022.4.56488. Clin Pract Cases Emerg Med. 2022. PMID: 36049190 Free PMC article.
-
Stroke Recurrence in Children with Vertebral Artery Dissecting Aneurysm.AJNR Am J Neuroradiol. 2022 Jun;43(6):913-918. doi: 10.3174/ajnr.A7518. Epub 2022 May 12. AJNR Am J Neuroradiol. 2022. PMID: 35550284 Free PMC article.
-
Hypoxic-ischemic injury causes functional and structural neurovascular degeneration in the juvenile mouse retina.Sci Rep. 2021 Jun 16;11(1):12670. doi: 10.1038/s41598-021-90447-5. Sci Rep. 2021. PMID: 34135369 Free PMC article.
-
Diagnosis and treatment of arterial dissections.Curr Neurol Neurosci Rep. 2014 Jan;14(1):419. doi: 10.1007/s11910-013-0419-3. Curr Neurol Neurosci Rep. 2014. PMID: 24272273 Review.
References
-
- Fullerton HJ, Johnston SC, Smith WS. Arterial dissection and stroke in children. Neurology. 2001;57:1155–1160. - PubMed
-
- Tan MA, Armstrong D, MacGregor DL, et al. Late complications of vertebral artery dissection in children: pseudoaneurysm, thrombosis, and recurrent stroke. J Child Neurol. 2009;24:354–360. - PubMed
-
- Fusco MR, Harrigan MR. Cerebrovascular dissections--a review part I: Spontaneous dissections. Neurosurgery. 2011;68:242–257. - PubMed
-
- Rafay MF, Armstrong D, DeVeber G, et al. Craniocervical arterial dissection in children: clinical and radiographic presentation and outcome. J Child Neurol. 2006;21:8–16. - PubMed
-
- Brandt T, Orberk E, Weber R, et al. Pathogenesis of cervical artery dissections: association with connective tissue abnormalities. Neurology. 2001;57:24–30. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
