

Transsinusoidal portal vein embolization with ethylene vinyl alcohol copolymer (Onyx): a feasibility study in pigs
- PMID: 21979794
- PMCID: PMC3447144
- DOI: 10.1007/s00270-011-0285-9
Transsinusoidal portal vein embolization with ethylene vinyl alcohol copolymer (Onyx): a feasibility study in pigs
Abstract
Purpose: Portal vein embolization is performed to increase the future liver remnant before liver surgery in patients with liver malignancies. This study assesses the feasibility of a transsinusoidal approach for portal vein embolization (PVE) with the ethylene vinyl alcohol copolymer, Onyx.
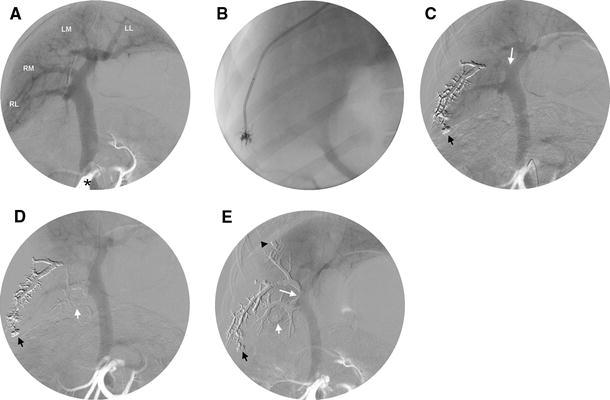
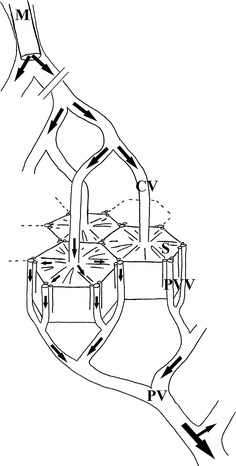
Methods: Indirect portography through contrast injection in the cranial mesenteric artery was performed in eight healthy pigs. Onyx was slowly injected through a microcatheter from a wedged position in the hepatic vein and advanced through the liver lobules into the portal system. The progression of Onyx was followed under fluoroscopy, and the extent of embolization was monitored by indirect portography. The pigs were euthanized immediately (n = 2), at 7 days (n = 4), or at 21 days postprocedure (n = 2). All pigs underwent necropsy and the ex vivo livers were grossly and histopathologically analyzed.
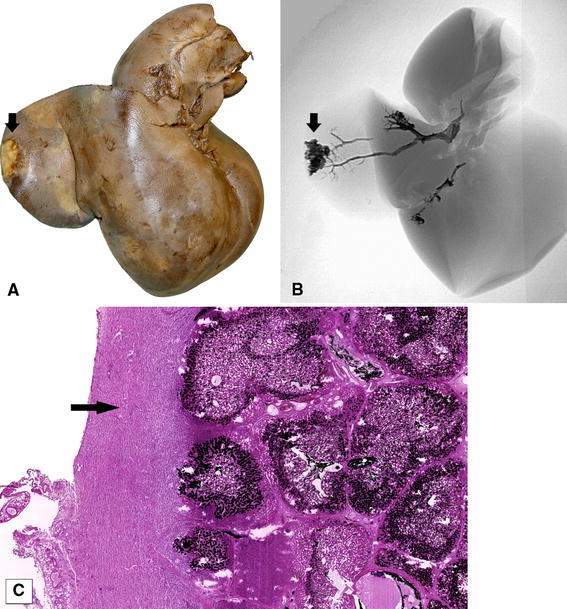
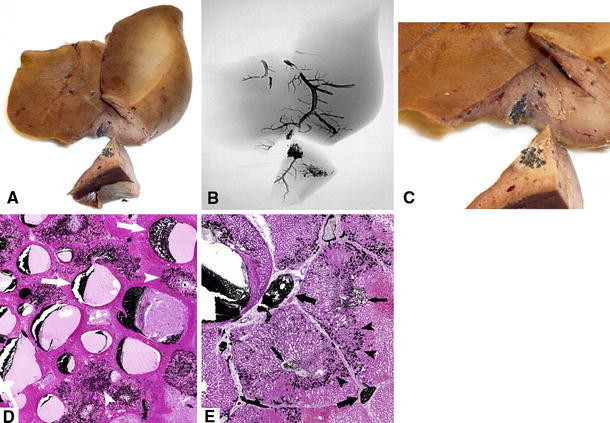
Results: Transsinusoidal PVE was successfully performed in five of eight pigs (63%). In 14 of 21 injections (67%), a segmental portal vein could be filled completely. A mean of 1.6 liver lobes per pig was embolized (range 1-2 lobes). There were no periprocedural adverse events. Focal capsular scarring was visible on the surface of two resected livers, yet the capsules remained intact. Histopathological examination showed no signs of recanalization or abscess formation. Mild inflammatory reaction to Onyx was observed in the perivascular parenchyma.
Conclusions: The porcine portal vein can be embolized through injection of Onyx from a wedged position in the hepatic vein. Possible complications of transsinusoidal PVE and the effect on contralateral hypertrophy need further study.
Figures
Similar articles
-
Transarterial versus transhepatic portal vein embolization to induce selective hepatic hypertrophy: a comparative study in swine.J Vasc Interv Radiol. 2007 Jan;18(1 Pt 1):79-93. doi: 10.1016/j.jvir.2006.10.018. J Vasc Interv Radiol. 2007. PMID: 17296708
-
Future liver remnant growth after various portal vein embolization regimens: a quantitative comparison.Minim Invasive Ther Allied Technol. 2020 Apr;29(2):98-106. doi: 10.1080/13645706.2019.1582067. Epub 2019 Mar 1. Minim Invasive Ther Allied Technol. 2020. PMID: 30821547
-
Comparison of four embolic materials for portal vein embolization: experimental study in pigs.Eur Radiol. 2009 Jun;19(6):1435-42. doi: 10.1007/s00330-008-1277-2. Epub 2009 Jan 20. Eur Radiol. 2009. PMID: 19153743
-
Preoperative portal vein embolization: indications and technical considerations.Tech Vasc Interv Radiol. 2007 Mar;10(1):67-78. doi: 10.1053/j.tvir.2007.08.003. Tech Vasc Interv Radiol. 2007. PMID: 17980321 Review.
-
A review of animal models for portal vein embolization.J Surg Res. 2014 Sep;191(1):179-88. doi: 10.1016/j.jss.2014.05.089. Epub 2014 Jun 6. J Surg Res. 2014. PMID: 25017706 Review.
Cited by
-
Transcatheter embolization with Squid, combined with other embolic agents or alone, in different abdominal diseases: a single-center experience in 30 patients.CVIR Endovasc. 2019 Feb 4;2(1):8. doi: 10.1186/s42155-019-0051-7. CVIR Endovasc. 2019. PMID: 32026992 Free PMC article.
-
Partial liver volume radioembolization induces hypertrophy in the spared hemiliver and no major signs of portal hypertension.HPB (Oxford). 2014 Mar;16(3):243-9. doi: 10.1111/hpb.12095. Epub 2013 Mar 27. HPB (Oxford). 2014. PMID: 23530966 Free PMC article.
-
Portal vein embolization with ethylene-vinyl alcohol copolymer for contralateral lobe hypertrophy before liver resection: safety, feasibility and initial experience.Quant Imaging Med Surg. 2021 Feb;11(2):797-809. doi: 10.21037/qims-20-808. Quant Imaging Med Surg. 2021. PMID: 33532278 Free PMC article.
-
Ethylene vinyl alcohol copolymer for occlusion of specific portal branches during preoperative portal vein embolisation with n-butyl-cyanoacrylate.Eur Radiol. 2018 Nov;28(11):4810-4817. doi: 10.1007/s00330-018-5476-1. Epub 2018 May 22. Eur Radiol. 2018. PMID: 29789913
-
Endohepatology: The endoscopic armamentarium in the hand of the hepatologist.Saudi J Gastroenterol. 2024 Jan 1;30(1):4-13. doi: 10.4103/sjg.sjg_214_23. Epub 2023 Nov 18. Saudi J Gastroenterol. 2024. PMID: 37988109 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
