

Abnormal haemodynamic response to exercise in heart failure with preserved ejection fraction
- PMID: 21979991
- PMCID: PMC3220394
- DOI: 10.1093/eurjhf/hfr133
Abnormal haemodynamic response to exercise in heart failure with preserved ejection fraction
Abstract
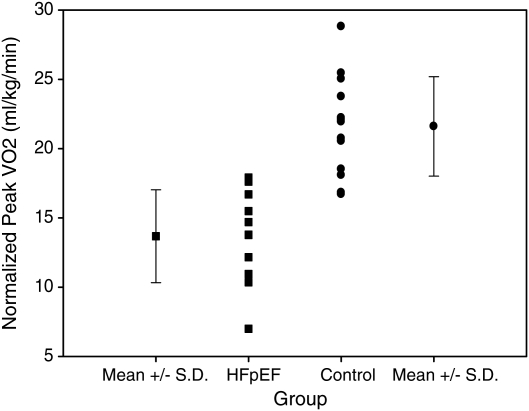
Aims: Peak oxygen uptake (VO(2)) is diminished in patients with heart failure with preserved ejection fraction (HFpEF) suggesting impaired cardiac reserve. To test this hypothesis, we assessed the haemodynamic response to exercise in HFpEF patients.
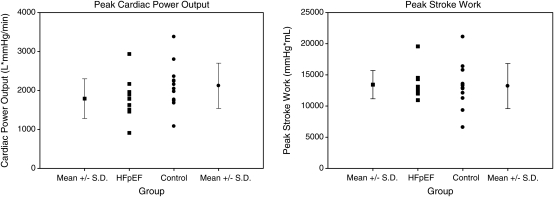
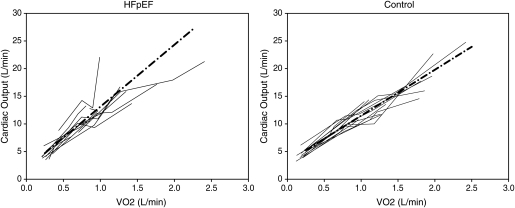
Methods and results: Eleven HFpEF patients (73 ± 7 years, 7 females/4 males) and 13 healthy controls (70 ± 4 years, 6 females/7 males) were studied during submaximal and maximal exercise. The cardiac output (Q(c), acetylene rebreathing) response to exercise was determined from linear regression of Q(c) and VO(2) (Douglas bags) at rest, ∼30% and ∼60% of peak VO(2), and maximal exercise. Peak VO(2) was lower in HFpEF patients than in controls (13.7 ± 3.4 vs. 21.6 ± 3.6 mL/kg/min; P < 0.001), while indices of cardiac reserve were not statistically different: peak cardiac power output [CPO = Q(c) × mean arterial pressure (MAP); HFpEF 1790 ± 509 vs. controls 2119 ± 581 L/mmHg/min; P = 0.20]; peak stroke work [SW = stroke volume (SV) × MAP; HFpEF 13 429 ± 2269 vs. controls 13 200 ± 3610 mL/mmHg; P = 0.80]. The ΔQ(c)/ΔVO(2) slope was abnormally elevated in HFpEF patients vs. controls (11.2 ±3.6 vs. 8.3 ± 1.5; P = 0.015).
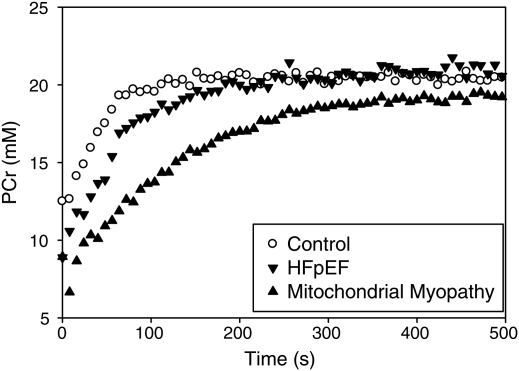
Conclusion: Contrary to our hypothesis, cardiac reserve is not significantly impaired in well-compensated outpatients with HFpEF. The abnormal haemodynamic response to exercise (decreased peak VO(2), increased ΔQ(c)/ΔVO(2) slope) is similar to that observed in patients with mitochondrial myopathies, suggesting an element of impaired skeletal muscle oxidative metabolism. This impairment may limit functional capacity by two mechanisms: (i) premature skeletal muscle fatigue and (ii) metabolic signals to increase the cardiac output response to exercise which may be poorly tolerated by a left ventricle with impaired diastolic function.
Figures
References
-
- Borlaug BA, Melenovsky V, Russell SD, Kessler K, Pacak K, Becker LC, Kass DA. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation. 2006;114:2138–2147. - PubMed
-
- Maeder MT, Thompson BR, Brunner-La Rocca H-P, Kaye DM. Hemodynamic basis of exercise limitation in patients with heart failure and normal ejection fraction. J Am Coll Cardiol. 2010;56:855–863. - PubMed
-
- Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure—abnormalities in active relaxation and passive stiffness of the left ventricle. N Engl J Med. 2004;350:1953–1959. - PubMed
-
- Westermann D, Kasner M, Steendijk P, Spillmann F, Riad A, Weitmann K, Hoffmann W, Poller W, Pauschinger M, Schultheiss H-P, Tschope C. Role of left ventricular stiffness in heart failure with normal ejection fraction. Circulation. 2008;117:2051–2060. - PubMed
-
- Willemsen S, Hartog JWL, Hummel YM, van Ruijven MHI, van der Horst ICC, van Veldhuisen DJ, Voors AA. Tissue advanced glycation end products are associated with diastolic function and aerobic exercise capacity in diabetic heart failure patients. Eur J Heart Fail. 2011;13:76–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
