

Decision making in patients with pulmonary nodules
- PMID: 21980032
- PMCID: PMC3361350
- DOI: 10.1164/rccm.201104-0679CI
Decision making in patients with pulmonary nodules
Abstract
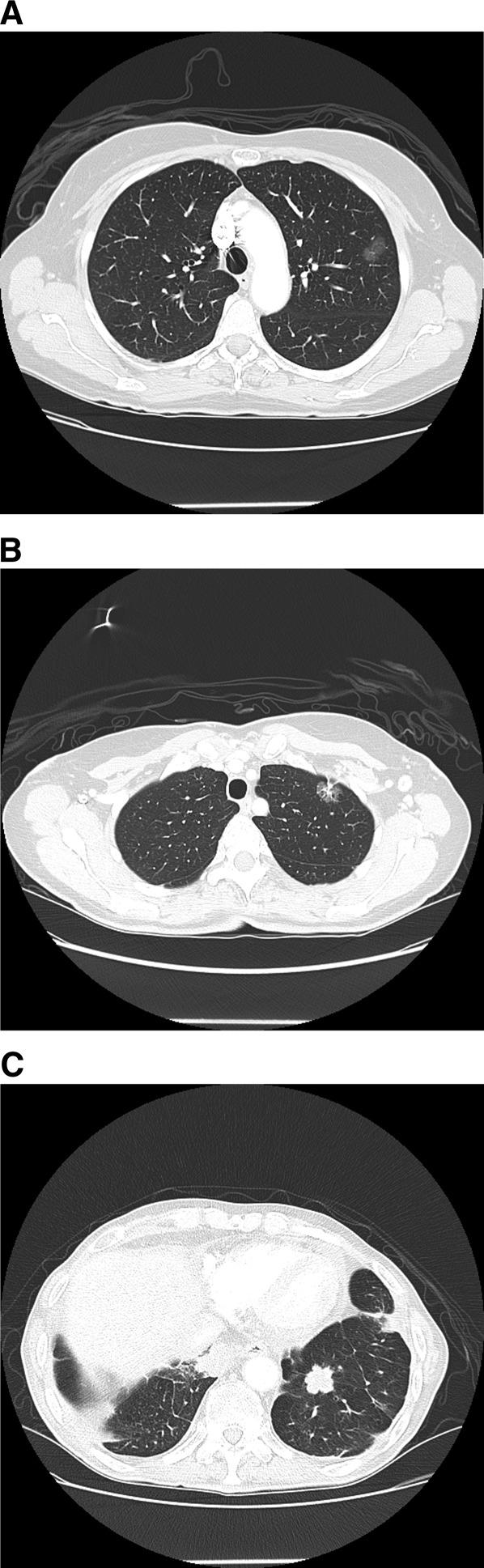
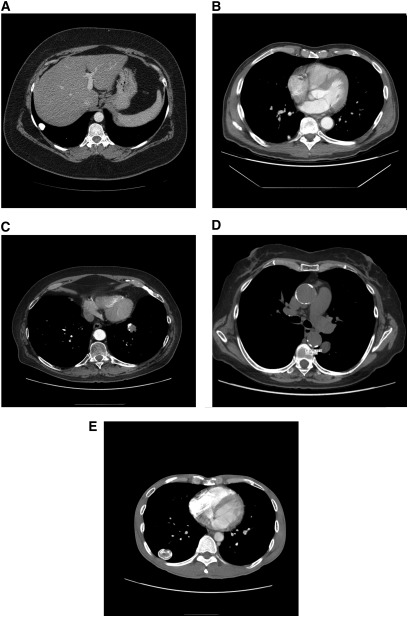
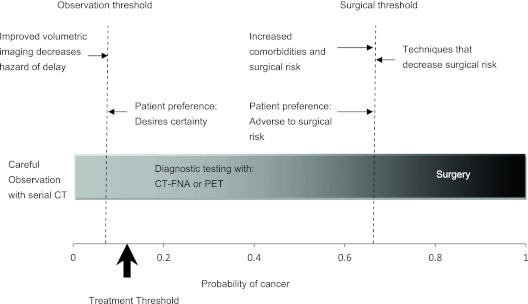
Integrating current evidence with fundamental concepts from decision analysis suggests that management of patients with pulmonary nodules should begin with estimating the pretest probability of cancer from the patient's clinical risk factors and computed tomography characteristics. Then, the consequences of treatment should be considered, by comparing the benefits of surgery if the patient has lung cancer with the potential harm if the patient does not have cancer. This analysis determines the "treatment threshold," which is the point around which the decision centers. This varies widely among patients depending on their cardiopulmonary reserve, comorbidities, and individual preferences. For patients with a very low probability of cancer, careful observation with serial computed tomography is warranted. For those with a high probability of cancer, surgical diagnosis is warranted. For patients in the intermediate range of probabilities, either computed tomography-guided fine-needle aspiration biopsy or positron emission tomography, possibly followed by computed tomography-guided fine-needle aspiration biopsy, is best. Patient preferences should be considered because the absolute difference in outcome between strategies may be small. The optimal approach to the management of patients with pulmonary nodules is evolving as technologies develop. Areas of uncertainty include quantifying the hazard of delayed diagnosis; determining the optimal duration of follow-up for ground-glass and semisolid opacities; establishing the roles of volumetric imaging, advanced bronchoscopic technologies, and limited surgical resections; and calculating the cost-effectiveness of different strategies.
Figures

References
-
- Ost D, Fein AM, Feinsilver SH. Clinical practice: the solitary pulmonary nodule. N Engl J Med 2003;348:2535–2542 - PubMed
-
- Swensen SJ, Morin RL, Schueler BA, Brown LR, Cortese DA, Pairolero PC, Brutinel WM. Solitary pulmonary nodule: CT evaluation of enhancement with iodinated contrast material—a preliminary report. Radiology 1992;182:343–347 - PubMed
-
- Swensen SJ, Jett JR, Payne WS, Viggiano RW, Pairolero PC, Trastek VF. An integrated approach to evaluation of the solitary pulmonary nodule. Mayo Clin Proc 1990;65:173–186 - PubMed
-
- Diederich S, Wormanns D, Semik M, Thomas M, Lenzen H, Roos N, Heindel W. Screening for early lung cancer with low-dose spiral CT: prevalence in 817 asymptomatic smokers. Radiology 2002;222:773–781 - PubMed
-
- McWilliams A, Mayo J, MacDonald S, leRiche JC, Palcic B, Szabo E, Lam S. Lung cancer screening: a different paradigm. Am J Respir Crit Care Med 2003;168:1167–1173 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
