

Screening, isolation, and decolonisation strategies in the control of meticillin resistant Staphylococcus aureus in intensive care units: cost effectiveness evaluation
- PMID: 21980062
- PMCID: PMC3188660
- DOI: 10.1136/bmj.d5694
Screening, isolation, and decolonisation strategies in the control of meticillin resistant Staphylococcus aureus in intensive care units: cost effectiveness evaluation
Abstract
Objective: To assess the cost effectiveness of screening, isolation, and decolonisation strategies in the control of meticillin resistant Staphylococcus aureus (MRSA) in intensive care units.
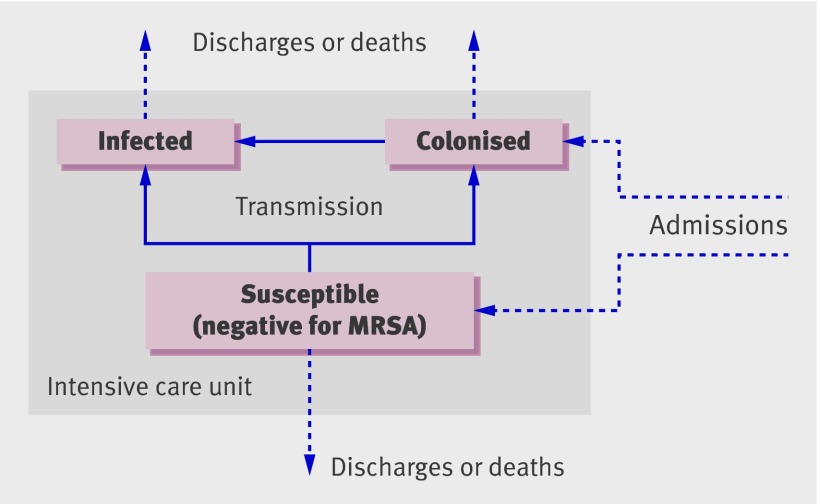
Design: Economic evaluation based on a dynamic transmission model.
Setting: England and Wales. Population Theoretical population of patients on an intensive care unit.
Main outcome measures: Infections, deaths, costs, quality adjusted life years (QALYs), incremental cost effectiveness ratios for alternative strategies, and net monetary benefits.
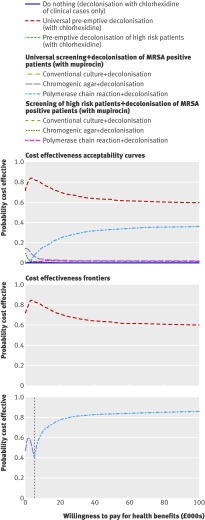
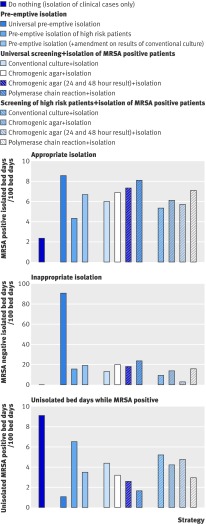
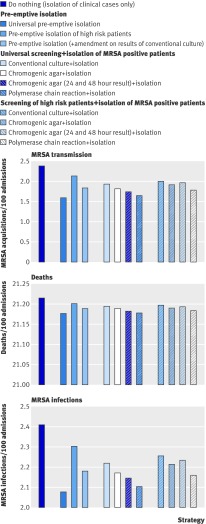
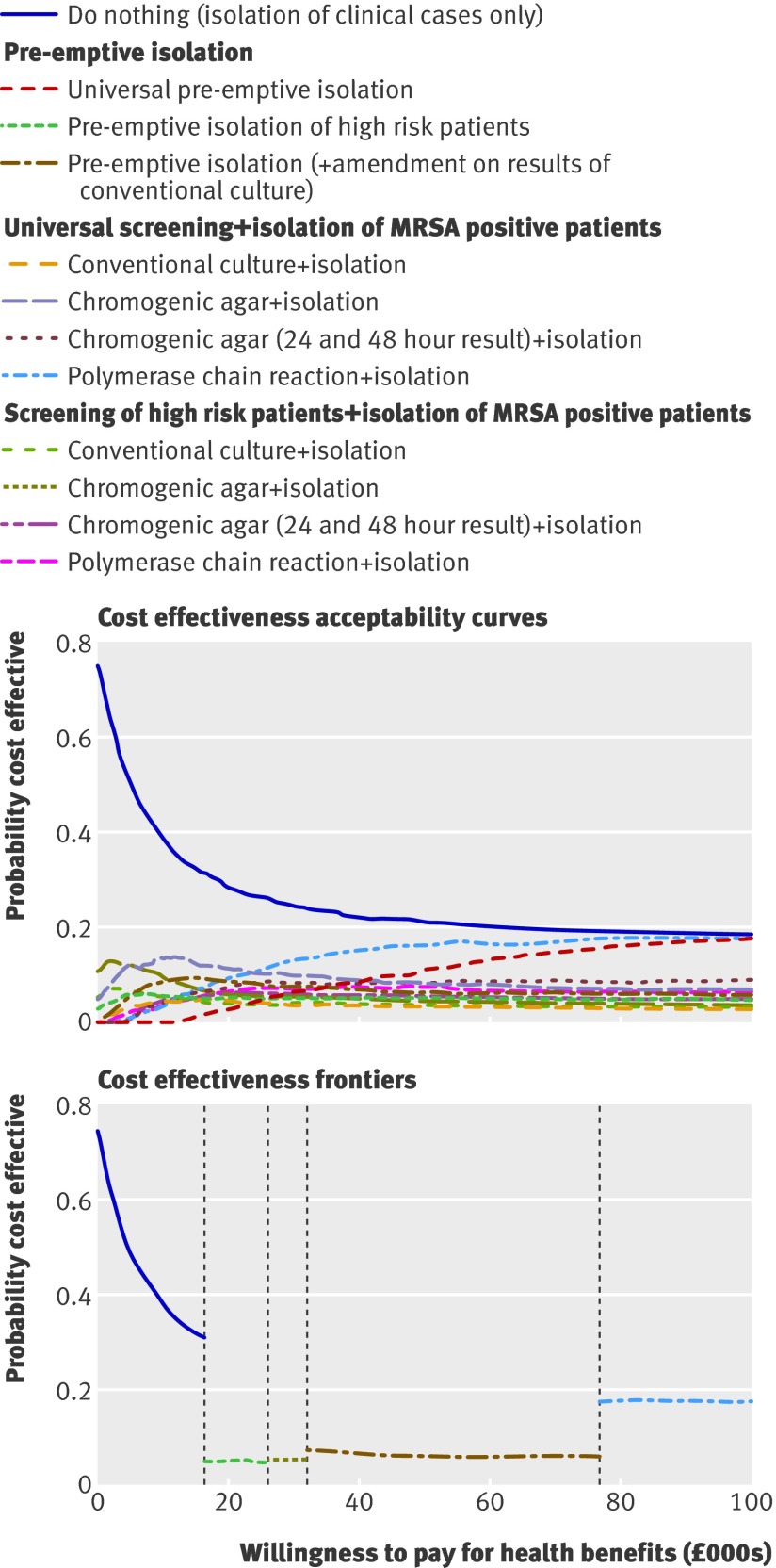
Results: All decolonisation strategies improved health outcomes and reduced costs. Although universal decolonisation (regardless of MRSA status) was the most cost effective in the short term, strategies using screening to target MRSA carriers may be preferred owing to the reduced risk of selecting for resistance. Among such targeted strategies, universal admission and weekly screening with polymerase chain reaction coupled with decolonisation using nasal mupirocin was the most cost effective. This finding was robust to the size of intensive care units, prevalence of MRSA on admission, proportion of patients classified as high risk, and precise value of willingness to pay for health benefits. All strategies using isolation but not decolonisation improved health outcomes but costs were increased. When the prevalence of MRSA on admission to the intensive care unit was 5% and the willingness to pay per QALY gained was between £20,000 (€23,000; $32,000) and £30,000, the best such strategy was to isolate only those patients at high risk of carrying MRSA (either pre-emptively or after identification by admission and weekly screening for MRSA using chromogenic agar). Universal admission and weekly screening using polymerase chain reaction based detection of MRSA coupled with isolation was unlikely to be cost effective unless prevalence was high (10% of patients colonised with MRSA on admission).
Conclusions: MRSA control strategies that use decolonisation are likely to be cost saving in an intensive care unit setting provided resistance is lacking, and combining universal screening using polymerase chain reaction with decolonisation is likely to represent good value for money if untargeted decolonisation is considered unacceptable. In intensive care units where decolonisation is not implemented, evidence is insufficient to support universal screening for MRSA outside high prevalence settings.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Control of MRSA in intensive care units.BMJ. 2011 Oct 5;343:d5885. doi: 10.1136/bmj.d5885. BMJ. 2011. PMID: 21980063 No abstract available.
References
-
- Cepeda JA, Whitehouse T, Cooper B, Hails J, Jones K, Kwaku F, et al. Isolation of patients in single rooms or cohorts to reduce spread of MRSA in intensive-care units: prospective two-centre study. Lancet 2005;365:295-304. - PubMed
-
- Bode LG, Kluytmans JA, Wertheim HF, Bogaers D, Vandenbroucke-Grauls CM, Roosendaal R, et al. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. N Engl J Med 2010;362:9-17. - PubMed
-
- Hardy K, Price C, Szczepura A, Gossain S, Davies R, Stallard N, et al. Reduction in the rate of methicillin-resistant Staphylococcus aureus acquisition in surgical wards by rapid screening for colonization: a prospective, cross-over study. Clin Microbiol Infect 2010;16:333-9. - PubMed
-
- Porter R, Subramani K, Thomas AN, Chadwick P. Nasal carriage of Staphylococcus aureus on admission to intensive care: incidence and prognostic significance. Intensive Care Med 2003;29:655-8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical