

Age and outcomes after carotid stenting and endarterectomy: the carotid revascularization endarterectomy versus stenting trial
- PMID: 21980205
- PMCID: PMC3312471
- DOI: 10.1161/STROKEAHA.111.624155
Age and outcomes after carotid stenting and endarterectomy: the carotid revascularization endarterectomy versus stenting trial
Abstract
Background and purpose: High stroke event rates among carotid artery stenting (CAS)-treated patients in the Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST) lead-in registry generated an a priori hypothesis that age may modify the relative efficacy of CAS versus carotid endarterectomy (CEA). In the primary CREST report, we previously noted significant effect modification by age. Here we extend this investigation by examining the relative efficacy of the components of the primary end point, the treatment-specific impact of age, and contributors to the increasing risk in CAS-treated patients at older ages.
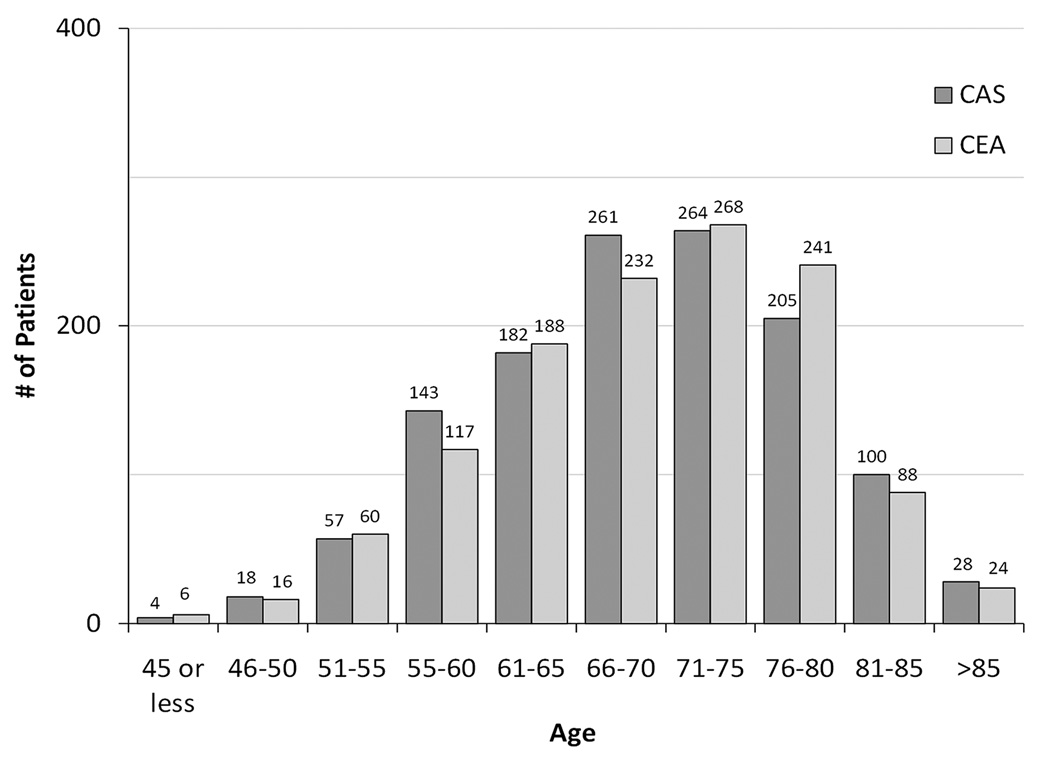
Methods: Among 2502 CREST patients with high-grade carotid stenosis, proportional hazards models were used to examine the impact of age on the CAS-to-CEA relative efficacy, and the impact of age on risk within CAS-treated and CEA-treated patients.
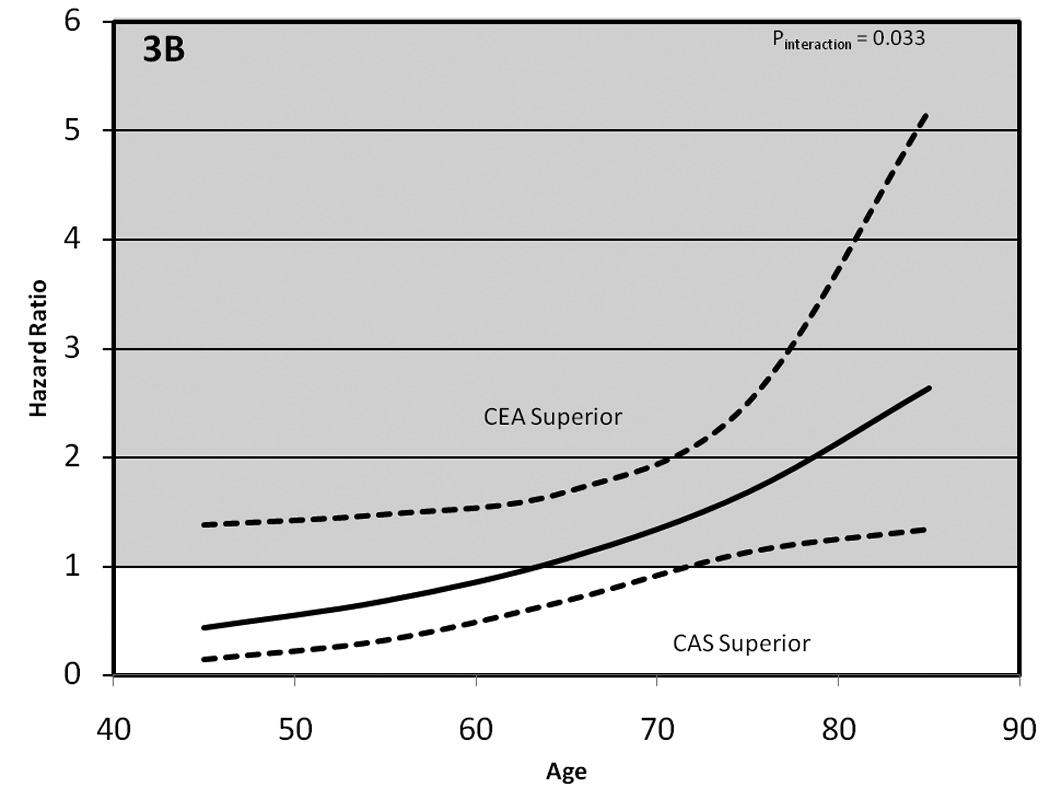
Results: Age acted as a treatment effect modifier for the primary end point (P interaction=0.02), with the efficacy of CAS and CEA approximately equal at age 70 years. For CAS, risk for the primary end point increased with age (P<0.0001) by 1.77-times (95% confidence interval, 1.38-2.28) per 10-year increment; however, there was no evidence of increased risk for CEA-treated patients (P=0.27). Stroke events were the primary contributor to the overall effect modification (P interaction=0.033), with equal risk at ≈64 years. The treatment-by-age interaction for CAS and CEA was not altered by symptomatic status (P=0.96) or by sex (P=0.45).
Conclusions: Outcomes after CAS versus CEA were related to patient age, attributable to increasing risk for stroke after CAS at older ages. Patient age should be an important consideration when choosing between the 2 procedures for treating carotid stenosis.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00004732.
Figures



References
-
- McCrory D, Goldstein L, Samsa G, Oddone E, Landsman P, Moore W, et al. Predicting complications of carotid endarterectomy. Stroke. 1993;24:1285–1291. - PubMed
-
- Durward QJ, Ragnarsson TS, Reeder RF, Case JL, Hughes CA. Carotid endarterectomy in nonagenarians. Arch Surg. 2005;140:625–628. - PubMed
-
- Salameh JR, Myers JL, Mukherjee D. Carotid Endarterectomy in Elderly Patients: Low Complication Rate With Overnight Stay. Arch Surg. 2002;137:1284–1287. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
