Surgical treatment of a parastomal hernia
- PMID: 21980587
- PMCID: PMC3180597
- DOI: 10.3393/jksc.2011.27.4.174
Surgical treatment of a parastomal hernia
Abstract
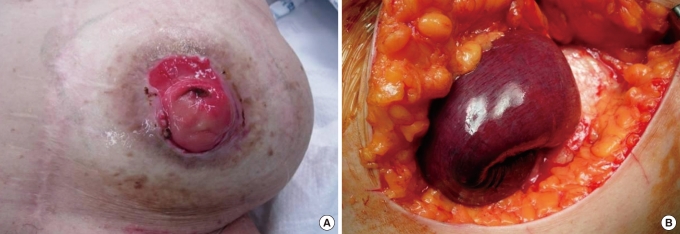
Purpose: Parastomal hernia is a major complication of an intestinal stoma. This study was performed to compare the results of various operative methods to treat parastomal hernias.
Methods: Results of surgical treatment for parastomal hernias (postoperative recurrence, complications and postoperative hospital stays) were surveyed in 39 patients over an 11-year period. The patients enrolled in this study underwent surgery by a single surgeon to exclude surgeon bias.
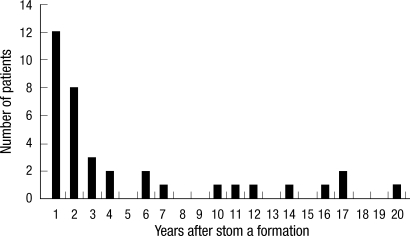
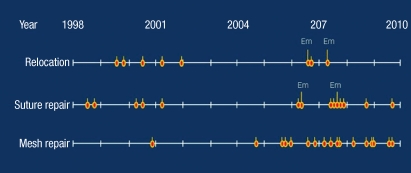
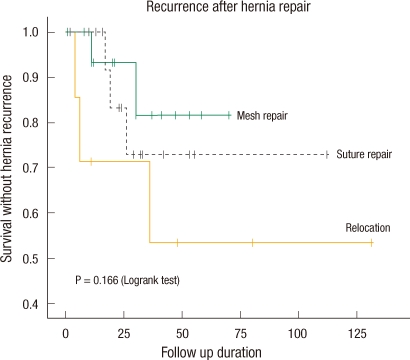
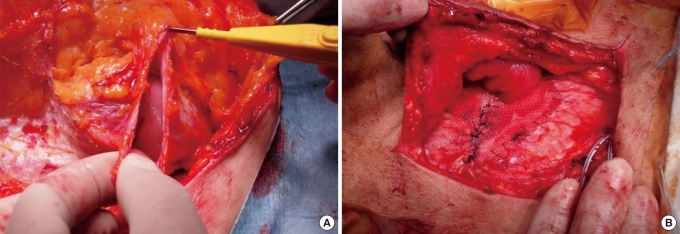
Results: Seventeen patients were male, and twenty-two patients were female. The mean age was 65.9 years (range, 36 to 86 years). The stomas were 35 sigmoid-end-colostomies (90%), 2 loop-colostomies (5%), and 2 double-barrel-colostomies. Over half of the hernias developed within two years after initial formation. Stoma relocation was performed in 8 patients, suture repair in 14 patients and mesh repair in 17 patients. Seven patients had recurrence of the hernia, and ten patients suffered from complications. Postoperative complications and recurrence were more frequent in stoma relocation than in suture repair and mesh repair. Emergency operations were performed in four patients (10.3%) with higher incidence of complications but not with increased risk of recurrence. Excluding emergency operations, complications of relocations were not higher than those of mesh repairs. Postoperative hospital stays were shortest in mesh repair patients.
Conclusion: In this study, mesh repair showed low recurrence and a low complication rate with shorter hospital stay than relocation methods, though these differences were not statistically significant. Further studies, including randomized trials, are necessary if more reliable data on the surgical treatment of parastomal hernias are to be obtained.
Keywords: Complication; Mesh repair; Parastomal hernia; Recurrence; Relocation.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Leong AP, Londono-Schimmer EE, Phillips RK. Life-table analysis of stomal complications following ileostomy. Br J Surg. 1994;81:727–729. - PubMed
-
- Londono-Schimmer EE, Leong AP, Phillips RK. Life table analysis of stomal complications following colostomy. Dis Colon Rectum. 1994;37:916–920. - PubMed
-
- Tekkis PP, Kocher HM, Payne JG. Parastomal hernia repair: modified thorlakson technique, reinforced by polypropylene mesh. Dis Colon Rectum. 1999;42:1505–1508. - PubMed
-
- Carne PW, Robertson GM, Frizelle FA. Parastomal hernia. Br J Surg. 2003;90:784–793. - PubMed
-
- Israelsson LA. Preventing and treating parastomal hernia. World J Surg. 2005;29:1086–1089. - PubMed
LinkOut - more resources
Full Text Sources