

Automated clinical reminders for primary care providers in the care of CKD: a small cluster-randomized controlled trial
- PMID: 21982456
- PMCID: PMC3221894
- DOI: 10.1053/j.ajkd.2011.08.028
Automated clinical reminders for primary care providers in the care of CKD: a small cluster-randomized controlled trial
Abstract
Background: Primary care physicians (PCPs) care for most non-dialysis-dependent patients with chronic kidney disease (CKD). Studies suggest that PCPs may deliver suboptimal CKD care. One means to improve PCP treatment of CKD is clinical decision support systems (CDSSs).
Study design: Cluster-randomized controlled trial.
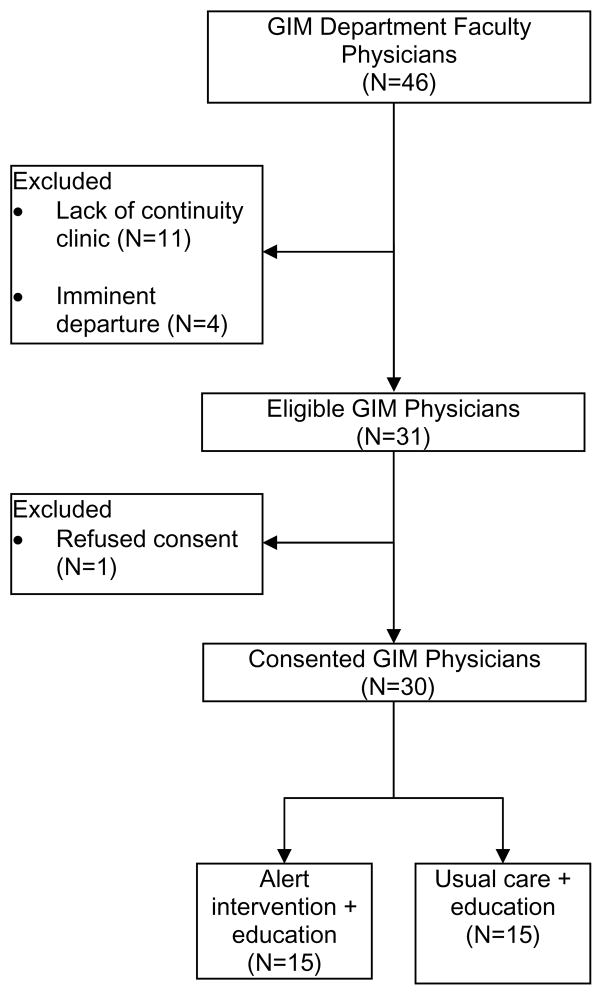
Setting & participants: 30 PCPs in a university-based outpatient general internal medicine practice and their 248 patients with moderate to advanced CKD who had not been referred to a nephrologist.
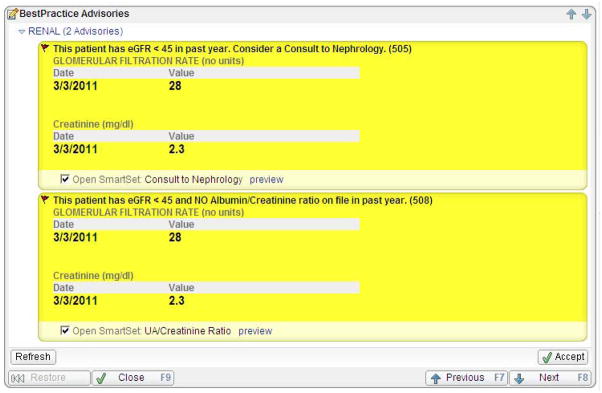
Intervention: 2 CKD educational sessions were held for PCPs in both arms. The 15 intervention-arm PCPs also received real-time automated electronic medical record alerts for patients with estimated glomerular filtration rates <45 mL/min/1.73 m(2) recommending renal referral and urine albumin quantification if not done within the prior year.
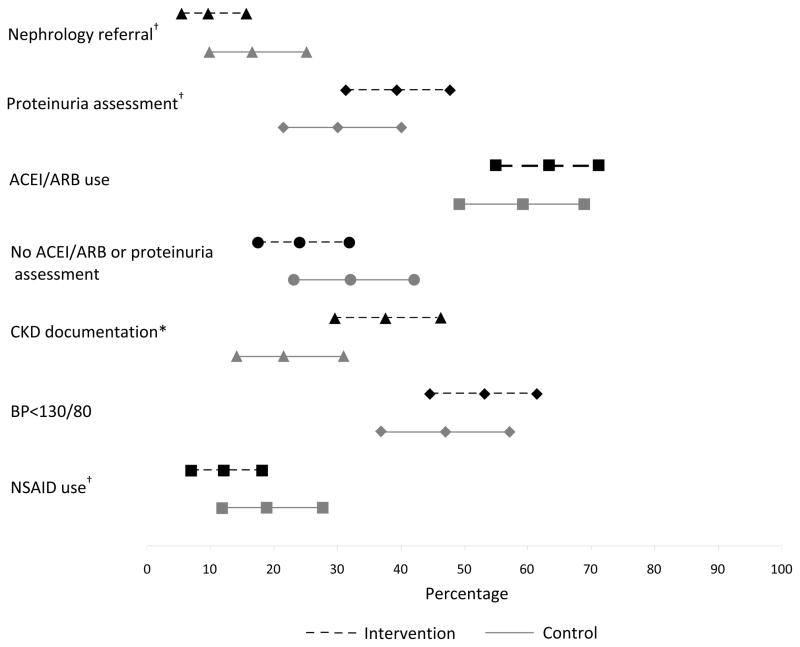
Outcomes: Primary outcome was referral to a nephrologist; secondary outcomes were albuminuria/proteinuria assessment, CKD documentation, optimal blood pressure (ie, <130/80 mm Hg), and use of renoprotective medications.
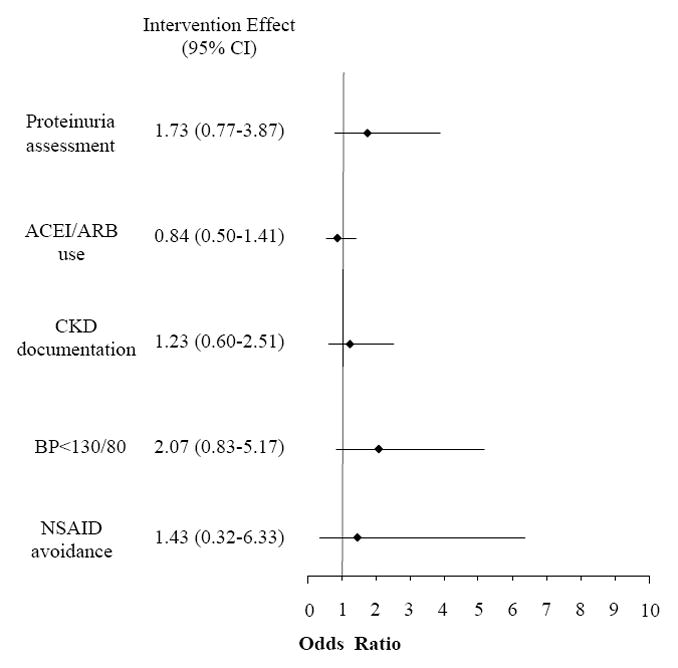
Results: The intervention and control arms did not differ in renal referrals (9.7% vs 16.5%, respectively; between-group difference, -6.8%; 95% CI, -15.5% to 1.8%; P = 0.1) or proteinuria assessments (39.3% vs 30.1%, respectively; between-group difference, 9.2%; 95% CI, -2.7% to 21.1%; P = 0.1). For intervention and control patients without a baseline proteinuria assessment, 27.7% versus 16.3%, respectively, had one at follow-up (P = 0.06). After controlling for clustering, these findings were largely unchanged and no significant differences were apparent between groups.
Limitations: Small single-center university-based practice, use of a passive CDSS that required PCPs to trigger the electronic order set.
Conclusions: PCPs were willing to partake in a randomized trial of a CDSS to improve outpatient CKD care. Although CDSSs may have potential, larger studies are needed to further explore how best to deploy them to enhance CKD care.
Trial registration: ClinicalTrials.gov NCT00688285.
Copyright © 2011 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Clinical decision support systems and the management of CKD by primary care physicians.Am J Kidney Dis. 2011 Dec;58(6):868-9. doi: 10.1053/j.ajkd.2011.10.003. Am J Kidney Dis. 2011. PMID: 22099568 No abstract available.
References
-
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038–2047. - PubMed
-
- Fields LE, Burt VL, Cutler JA, Hughes J, Roccella EJ, Sorlie P. The burden of adult hypertension in the United States 1999 to 2000: a rising tide. Hypertension. 2004;44(4):398–404. - PubMed
-
- Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999–2000. JAMA. 2002;288(14):1723–1727. - PubMed
-
- Gregg EW, Cheng YJ, Narayan KM, Thompson TJ, Williamson DF. The relative contributions of different levels of overweight and obesity to the increased prevalence of diabetes in the United States: 1976–2004. Prev Med. 2007;45(5):348–352. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
