

Impact of healthcare-associated acquisition on community-onset Gram-negative bloodstream infection: a population-based study: healthcare-associated Gram-negative BSI
- PMID: 21983895
- PMCID: PMC3369543
- DOI: 10.1007/s10096-011-1424-6
Impact of healthcare-associated acquisition on community-onset Gram-negative bloodstream infection: a population-based study: healthcare-associated Gram-negative BSI
Abstract
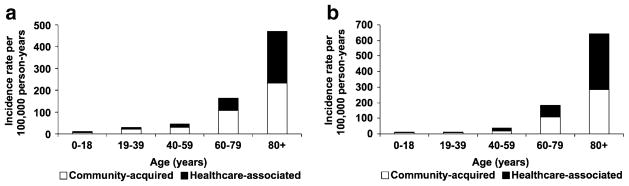
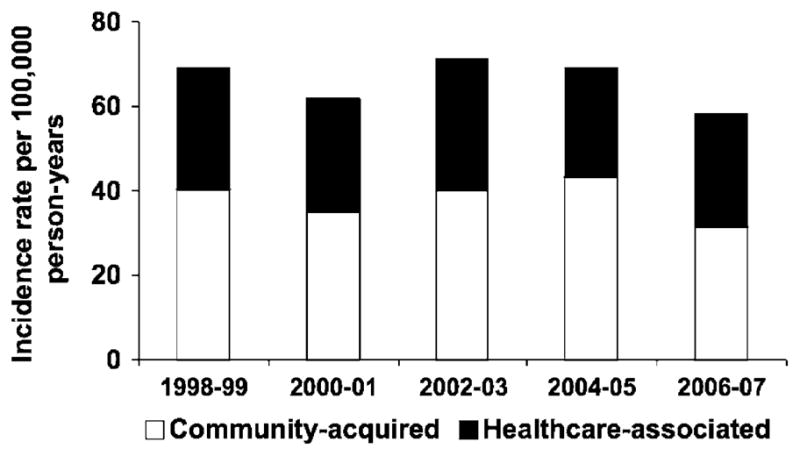
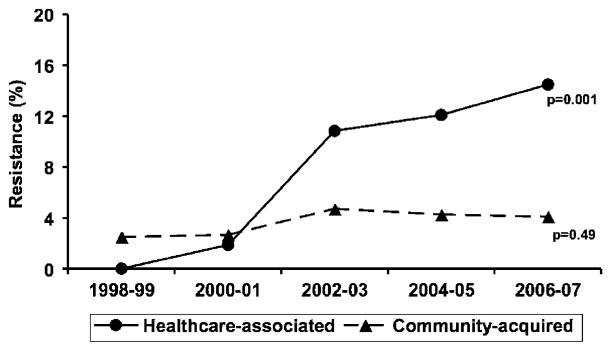
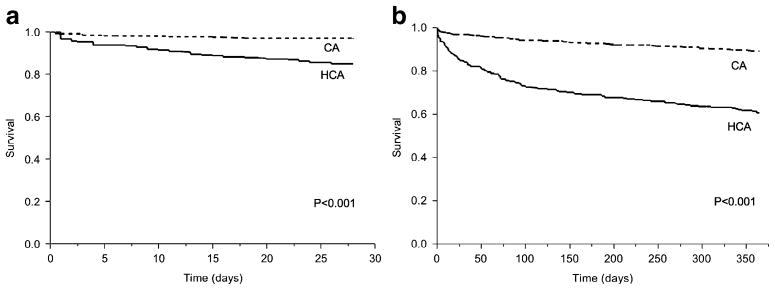
We performed a population-based study to examine the influence of healthcare-associated acquisition on pathogen distribution, antimicrobial resistance, short- and long-term mortality of community-onset Gram-negative bloodstream infections (BSI). We identified 733 unique patients with community-onset Gram-negative BSI (306 healthcare-associated and 427 community-acquired) among Olmsted County, Minnesota, residents from 1 January 1998 to 31 December 2007. Multivariate logistic regression was used to examine the association between healthcare-associated acquisition and microbiological etiology and antimicrobial resistance. Multivariate Cox proportional hazards regression was used to evaluate the influence of the site of acquisition on mortality. Healthcare-associated acquisition was predictive of Pseudomonas aeruginosa (odds ratio [OR] 3.14, 95% confidence intervals [CI]: 1.59-6.57) and the group of Enterobacter, Citrobacter, and Serratia species (OR 2.23, 95% CI: 1.21-4.21) as causative pathogens of community-onset Gram-negative BSI. Healthcare-associated acquisition was also predictive of fluoroquinolone resistance among community-onset Gram-negative bloodstream isolates (OR 2.27, 95% CI: 1.18-4.53). Healthcare-associated acquisition of BSI was independently associated with higher 28-day (hazard ratio [HR] 3.73, 95% CI: 2.13-6.93) and 1-year mortality (HR 3.60, 95% CI: 2.57-5.15). Because of differences in pathogen distribution, antimicrobial resistance, and outcomes between healthcare-associated and community-acquired Gram-negative BSI, identification of patients with healthcare-associated acquisition of BSI is essential to optimize empiric antimicrobial therapy.
Conflict of interest statement
Figures
References
-
- Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC definitions for nosocomial infections, 1988. Am J Infect Control. 1988;16:128–140. - PubMed
-
- Friedman ND, Kaye KS, Stout JE, McGarry SA, Trivette SL, Briggs JP, et al. Health care-associated bloodstream infections in adults: a reason to change the accepted definition of community-acquired infections. Ann Intern Med. 2002;137:791–797. - PubMed
-
- Shorr AF, Tabak YP, Killian AD, Gupta V, Liu LZ, Kollef MH. Healthcare-associated bloodstream infection: a distinct entity? Insights from a large U.S. database. Crit Care Med. 2006;34:2588–2595. - PubMed
-
- Marschall J, Fraser VJ, Doherty J, Warren DK. Between community and hospital: healthcare-associated Gram-negative bacteremia among hospitalized patients. Infect Control Hosp Epidemiol. 2009;30:1050–1056. - PubMed
-
- Olesen B, Kolmos HJ, Orskov F, Orskov I. A comparative study of nosocomial and community-acquired strains of Escherichia coli causing bacteraemia in a Danish University Hospital. J Hosp Infect. 1995;31:295–304. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
