

Comparison of laparoscopic anterior discoid resection and laparoscopic low anterior resection of deep infiltrating rectosigmoid endometriosis
- PMID: 21985719
- PMCID: PMC3183552
- DOI: 10.4293/108680811X13125733356431
Comparison of laparoscopic anterior discoid resection and laparoscopic low anterior resection of deep infiltrating rectosigmoid endometriosis
Abstract
Objective: To compare laparoscopic anterior discoid resection (ADR) with low anterior resection (LAR).
Methods: This is a retrospective review of a cohort (Canadian Task Force classification II-2) of patients undergoing laparoscopic ADR or LAR at a university hospital. Chart review and telephone questionnaires were conducted to examine long-term outcomes. Preoperative and operative findings, short- and long-term outcomes were compared. SF-12 quality of life scores, need for further interventions, and overall satisfaction were also compared.
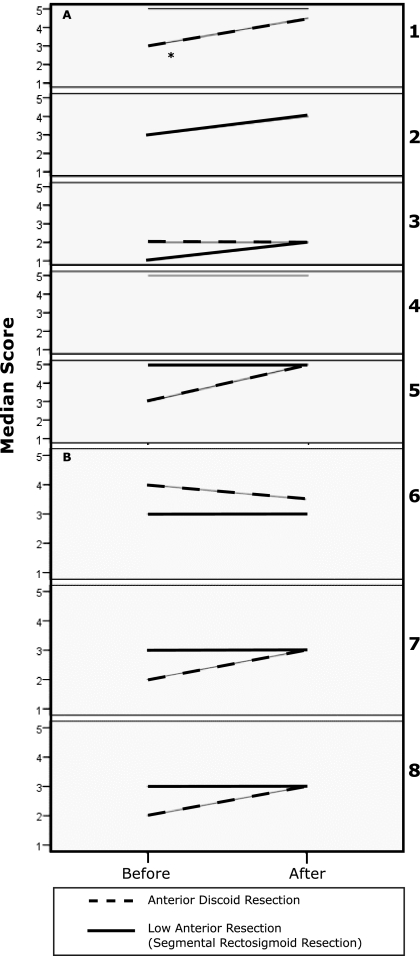
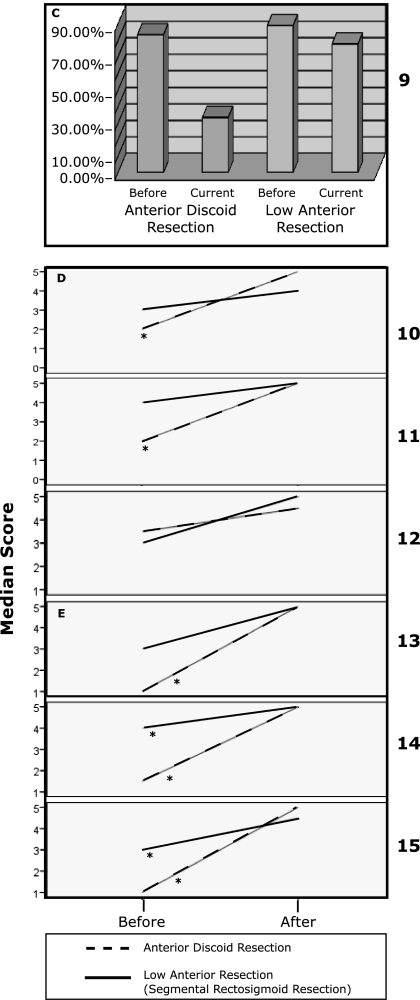
Results: Twenty-two patients underwent laparoscopic ADR (n 8) or LAR (n 14) for rectosigmoid endometriosis between January 2001 and December 2009. Mean follow-up time was 41.26 months (range, 14 to 70). Patients undergoing laparoscopic ADR had significantly less blood loss and shorter operative time and hospital stay. Patients who required LAR had a significantly higher rate of mucosal involvement (61.5% v. 0%). No statistically significant difference was found in the size, depth of invasion, location of lesions, or operative complications. Fifty percent of the LAR group had several lesions as opposed to 12.5% of the ADR group. Median age was significantly higher in patients who required LAR (39) than in patients who required ADR (32). Three patients in the LAR group (21.4%) had anastomotic strictures; 2 required dilation. The ADR group had consistently higher increments of improvement in bowel symptoms and dyspareunia. Overall satisfaction rate with the procedures was 93.3%. SF-12 scores were comparable between the 2 groups.
Conclusion: ADR compared with LAR is associated with decreased operative time, blood loss, and hospital stay and a lower rate of anastomotic strictures. Other outcomes and satisfaction rates are comparable between the 2 procedures.
Figures
References
-
- Weed JC, Ray JE. Endometriosis of the bowel. Obstet Gynecol. 1987; 69: 727–730 - PubMed
-
- Redwine DB. Variations in tubal configuration in endometriosis? Fertil Steril. 2006; 85: 267; author reply 267 - PubMed
-
- Nezhat C, Nezhat F, Pennington E, Nezhat CH, Ambroze W. Laparoscopic disk excision and primary repair of the anterior rectal wall for the treatment of full-thickness bowel endometriosis. Surg Endosc. 1994; 8: 682–685 - PubMed
-
- Ponka JL, Brush BE, Hodgkinson CP. Colorectal endometriosis. Dis Colon Rectum. 1973; 16: 490–499 - PubMed
-
- Prystowsky JB, Stryker SJ, Ujiki GT, Poticha SM. Gastrointestinal endometriosis. Incidence and indications for resection. Arch Surg. 1988; 123: 855–858 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous