

The effect of hepatic lipase on coronary artery disease in humans is influenced by the underlying lipoprotein phenotype
- PMID: 21986251
- PMCID: PMC3288605
- DOI: 10.1016/j.bbalip.2011.09.008
The effect of hepatic lipase on coronary artery disease in humans is influenced by the underlying lipoprotein phenotype
Abstract
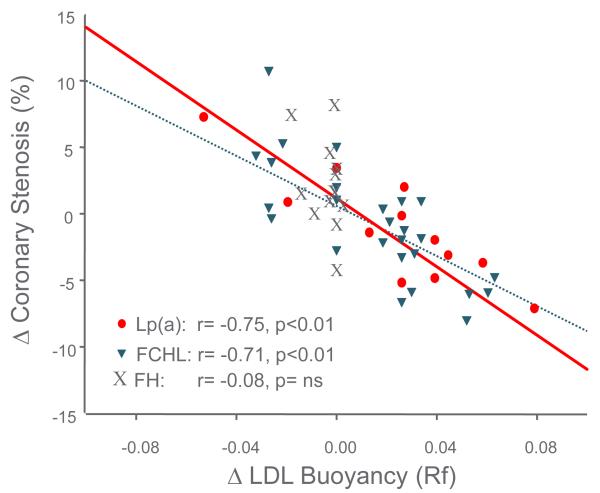
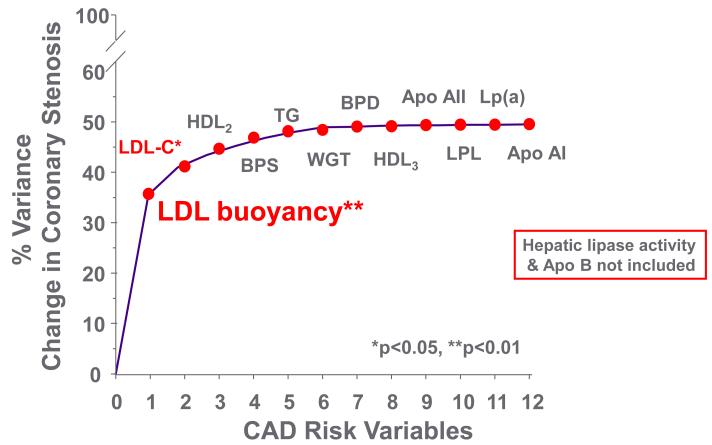
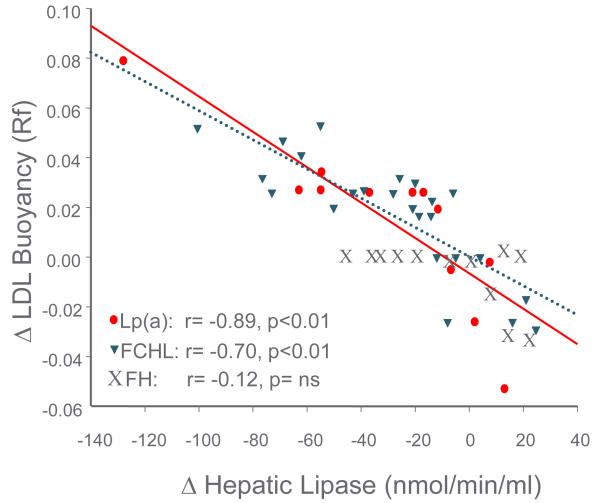
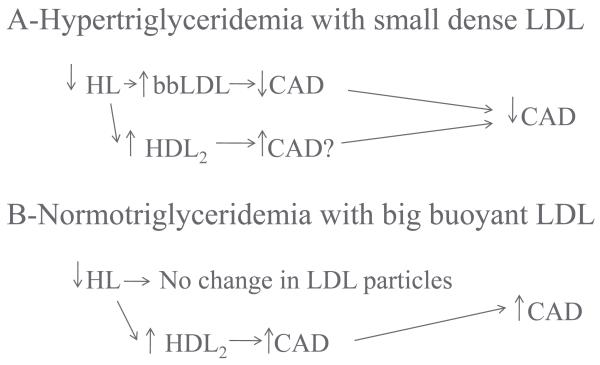
Increased or decreased hepatic lipase (HL) activity has been associated with coronary artery disease (CAD). This is consistent with the findings that gene variants that influence HL activity were associated with increased CAD risk in some population studies but not in others. In this review, we will explain the conditions that influence the effects of HL on CAD. Increased HL is associated with smaller and denser LDL (sdLDL) and HDL (HDL(3)) particles, while decreased HL is associated with larger and more buoyant LDL and HDL particles. The effect of HL activity on CAD risk is dependent on the underlying lipoprotein phenotype or disorder. Central obesity with hypertriglyceridemia (HTG) is associated with high HL activity that leads to the formation of sdLDL that is pro-atherogenic. In the absence of HTG, where large buoyant cholesteryl ester-enriched LDL is prominent, elevation of HL does not raise the risk for CAD. In HTG patients, drug therapy that decreases HL activity selectively decreases sdLDL particles, an anti-atherogenic effect. Drug therapy that raises HDL(2) cholesterol has not decreased the risk for CAD. In trials where inhibition of cholesterol ester transfer protein (CETP) or HL occurs, the increase in HDL(2) most likely is due to inhibition of catabolism of HDL(2) and impairment of reverse cholesterol transport (RCT). In patients with isolated hypercholesterolemia, but with normal triglyceride levels and big-buoyant LDL particles, an increase in HL activity is beneficial; possibly because it increases RCT. Drugs that lower HL activity might decrease the risk for CAD only in hypertriglyceridemic patients with sdLDL by selectively clearing sdLDL particles from plasma, which would override the potentially pro-atherogenic effect on RCT. This article is part of a Special Issue entitled Advances in High Density Lipoprotein Formation and Metabolism: A Tribute to John F. Oram (1945-2010).
Copyright © 2011 Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Contribution of the hepatic lipase gene to the atherogenic lipoprotein phenotype in familial combined hyperlipidemia.J Lipid Res. 2000 Feb;41(2):245-52. J Lipid Res. 2000. PMID: 10681408
-
Contribution of hepatic lipase, lipoprotein lipase, and cholesteryl ester transfer protein to LDL and HDL heterogeneity in healthy women.Arterioscler Thromb Vasc Biol. 2002 Apr 1;22(4):667-73. doi: 10.1161/01.atv.0000013284.47317.95. Arterioscler Thromb Vasc Biol. 2002. PMID: 11950708
-
Smaller low-density lipoprotein size as a possible risk factor for the prevalence of coronary artery diseases in haemodialysis patients: associations of cholesteryl ester transfer protein and the hepatic lipase gene polymorphism with low-density lipoprotein size.Nephrology (Carlton). 2011 Aug;16(6):558-66. doi: 10.1111/j.1440-1797.2011.01454.x. Nephrology (Carlton). 2011. PMID: 21352420
-
Hepatic lipase deficiency.Crit Rev Clin Lab Sci. 1998 Dec;35(6):547-72. doi: 10.1080/10408369891234273. Crit Rev Clin Lab Sci. 1998. PMID: 9885775 Review.
-
Clinical relevance of the biochemical, metabolic, and genetic factors that influence low-density lipoprotein heterogeneity.Am J Cardiol. 2002 Oct 17;90(8A):30i-47i. doi: 10.1016/s0002-9149(02)02749-2. Am J Cardiol. 2002. PMID: 12419479 Review.
Cited by
-
HDL in CKD: how good is the "good cholesterol?".J Am Soc Nephrol. 2014 May;25(5):871-4. doi: 10.1681/ASN.2014010062. Epub 2014 Mar 7. J Am Soc Nephrol. 2014. PMID: 24610924 Free PMC article. No abstract available.
-
Estimated sdLDL-C for predicting high-risk coronary plaque features in psoriasis: a prospective observational study.Lipids Health Dis. 2023 Apr 27;22(1):55. doi: 10.1186/s12944-023-01819-x. Lipids Health Dis. 2023. PMID: 37106374 Free PMC article.
-
The Relationship Between Lipoproteins and Insulin Sensitivity in Youth With Obesity and Abnormal Glucose Tolerance.J Clin Endocrinol Metab. 2022 May 17;107(6):1541-1551. doi: 10.1210/clinem/dgac113. J Clin Endocrinol Metab. 2022. PMID: 35240684 Free PMC article.
-
Carotid Intima-media Thickness and Small Dense Low-density Lipoprotein Cholesterol Increase after One Year of Treatment with Direct-acting Antivirals in Patients with Hepatitis C Virus Infection.Intern Med. 2019 May 1;58(9):1209-1215. doi: 10.2169/internalmedicine.1514-18. Epub 2019 Jan 10. Intern Med. 2019. PMID: 30626818 Free PMC article.
-
Dietary Fat Intake Modifies the Effect of a Common Variant in the LIPC Gene on Changes in Serum Lipid Concentrations during a Long-Term Weight-Loss Intervention Trial.J Nutr. 2015 Jun;145(6):1289-94. doi: 10.3945/jn.115.212514. Epub 2015 Apr 29. J Nutr. 2015. PMID: 25926410 Free PMC article. Clinical Trial.
References
-
- Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364:937–952. - PubMed
-
- Lamarche B, Moorjani S, Cantin B, Dagenais GR, Lupien PJ, Despres JP, Prospective results from the Quebec Cardiovascular Study Associations of HDL2 and HDL3 subfractions with ischemic heart disease in men. Arterioscler Thromb Vasc Biol. 1997;17:1098–1105. - PubMed
-
- Lamarche B, Tchernof A, Moorjani S, Cantin B, Dagenais GR, Lupien PJ, Despres JP, Prospective results from the Quebec Cardiovascular Study Small, dense low-density lipoprotein particles as a predictor of the risk of ischemic heart disease in men. Circulation. 1997;95:69–75. - PubMed
-
- Musunuru K, Orho-Melander M, Caulfield MP, Li S, Salameh WA, Reitz RE, Berglund G, Hedblad B, Engstrom G, Williams PT, Kathiresan S, Melander O, Krauss RM. Ion mobility analysis of lipoprotein subfractions identifies three independent axes of cardiovascular risk. Arterioscler Thromb Vasc Biol. 2009;29:1975–1980. - PMC - PubMed
-
- Deeb S, Peng R. Structure of the human lipoprotein lipase gene. Biochemistry. 1989;28:4131–4135. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
