

Distribution of cavitations as identified with accelerometry during lumbar spinal manipulation
- PMID: 21986305
- PMCID: PMC3215819
- DOI: 10.1016/j.jmpt.2011.05.015
Distribution of cavitations as identified with accelerometry during lumbar spinal manipulation
Abstract
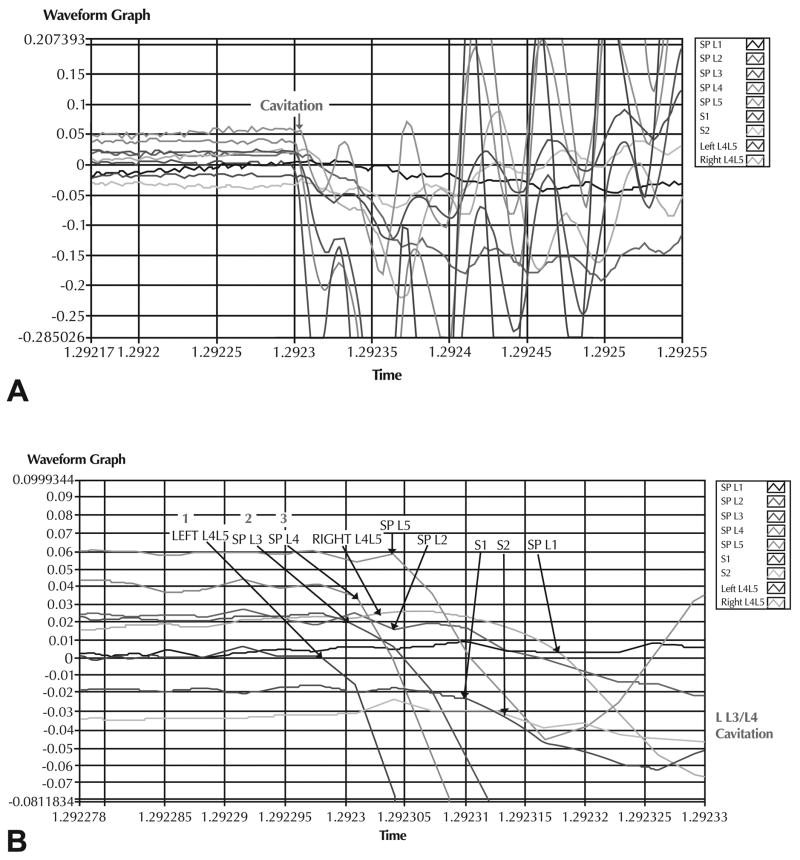
Objective: This project determined the location and distribution of cavitations (producing vibrations and audible sounds) in the lumbar zygapophyseal (Z) joints that were targeted by spinal manipulative therapy (SMT).
Methods: This randomized, controlled, clinical study assessed 40 healthy subjects (20 men, 20 women) 18 to 30 years of age who were block randomized into SMT (group 1, n = 30) or side-posture positioning only (group 2; control, n = 10) groups. Nine accelerometers were placed on each patient (7 on spinous processes/sacral tubercles of L1-S2 and 2 placed 3 cm left and right lateral to the L4/L5 interspinous space). Accelerometer recordings were made during side-posture positioning (groups 1 and 2) and SMT (group 1 only). The SMT was delivered by a chiropractic physician with 19 years of practice experience and included 2 high-velocity, low-amplitude thrusts delivered in rapid succession. Comparisons using χ(2) or McNemar test were made between number of joints cavitating from group 1 vs group 2, upside (contact side for SMT) vs downside, and Z joints within the target area (L3/L4, L4L5, L5/S1) vs outside the target area (L1/L2, L2/L3, sacroiliac).
Results: Fifty-six cavitations were recorded from 46 joints of 40 subjects. Eight joints cavitated more than once. Group 1 joints cavitated more than group 2 joints (P < .0001), upside joints cavitated more than downside joints (P < .0001), and joints inside the target area cavitated more than those outside the target area (P < .01).
Conclusions: Most cavitations (93.5%) occurred on the upside of SMT subjects in segments within the target area (71.7%). As expected, SMT subjects cavitated more frequently than did subjects with side-posture positioning only (96.7% vs 30%). Multiple cavitations from the same Z joints had not been previously reported.
Copyright © 2011 National University of Health Sciences. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
No conflicts of interest were reported for this study.
Figures





References
-
- Conway P, Herzog W, Zhang Y, Hasler E. Identification of the mechanical factors required to cause cavitation during spinal manipulation in the thoracic spine. International Conference on Spinal Manipulation; 1992 May 15–17; Chicago, IL. pp. 281–4.
-
- Conway P, Herzog W, Zhang Y, Hasler E. Forces required to cause cavitation during spinal manipulation of the thoracic spine. Clinical Biomechanics. 1993;8:210–4. - PubMed
-
- Ross JK, Bereznick DE, McGill SM. Determining cavitation location during lumbar and thoracic spinal manipulation: is spinal manipulation accurate and specific? Spine. 2004;29(13):1452–7. - PubMed
-
- Mierau D, Cassidy JD, Bowen V, Dupuis B, Noftall F. Manipulation and mobilization of the third metacarpophalangeal joint: a quantitative radiographic and range of motion study. Manual Med. 1988;3:135–40.
-
- Brodeur R. The audible release associated with joint manipulation. J Manipulative Physiol Ther. 1995;18(3):155–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
