

Management of the complications of endoscopic submucosal dissection
- PMID: 21987602
- PMCID: PMC3180012
- DOI: 10.3748/wjg.v17.i31.3575
Management of the complications of endoscopic submucosal dissection
Abstract
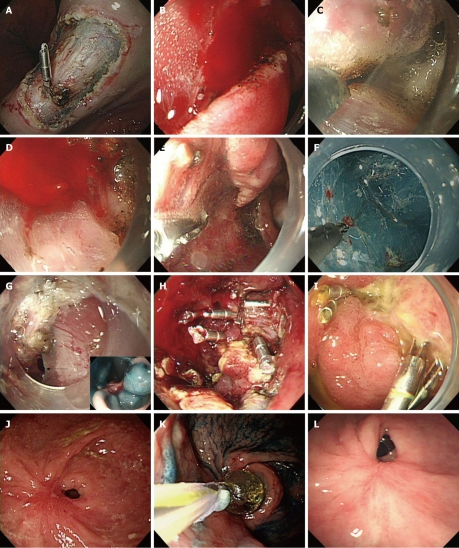
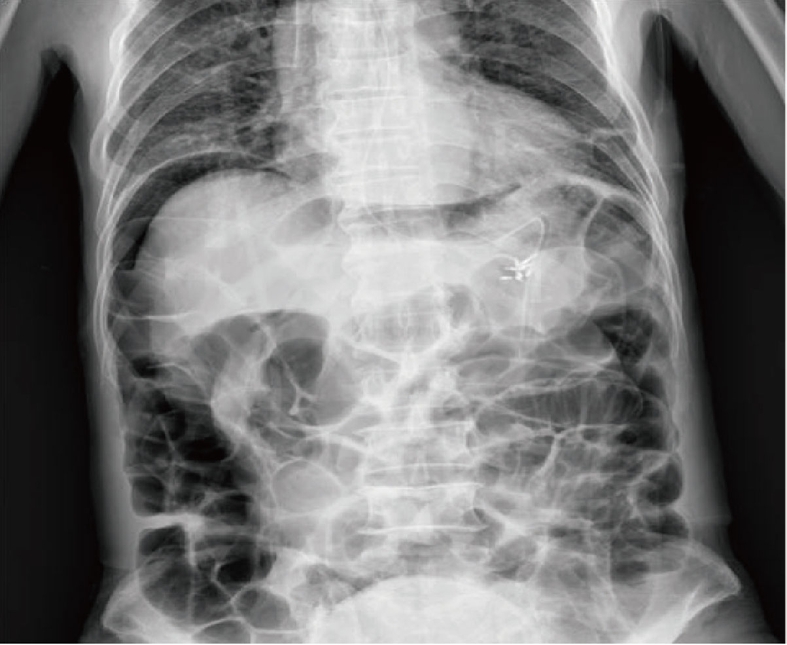
Endoscopic submucosal dissection (ESD) is currently widely accepted as a standard treatment option for early gastrointestinal neoplasms in Korea. However, ESD has technical difficulties and a longer procedure time than conventional endoscopic resection. So it may have a higher risk of complications than conventional endoscopic resection techniques. We, the ESD study group of Korean Society of Gastrointestinal Endoscopy, have experienced many complications, mostly treated by endoscopic or conservative management. Here, we introduce and share our experiences for management of post ESD complications and review published papers on the topic.
Keywords: Complication; Endoscopic submucosal dissection; Management.
Figures
References
-
- Cho JY, Jin SY, Shim CS. Neresection of early gastric cancer-endoscopic incision & submucosal dissection. 1st ed. Seoul: Jin; 2006.
-
- Kim SG. Endoscopic manipulation of complications. Korean J Gastrointest Endosc. 2007;35 Suppl 1:S65–S69.
-
- Kim JJ. The management of the complications in the endoscopic mucosal resection-prevention and treatment. Korean J Gastrointest Endosc. 2006;32 Suppl 1:S125–S129.
-
- Toyonaga T. ESD atlas-selection of devices and capture method according to the region. 1st ed. Seoul: Hankuk; 2007.
-
- Saito Y, Uraoka T, Matsuda T, Emura F, Ikehara H, Mashimo Y, Kikuchi T, Fu KI, Sano Y, Saito D. Endoscopic treatment of large superficial colorectal tumors: a case series of 200 endoscopic submucosal dissections (with video) Gastrointest Endosc. 2007;66:966–973. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
