

Gain of chromosome arm 1q in atypical meningioma correlates with shorter progression-free survival
- PMID: 21988727
- PMCID: PMC3563294
- DOI: 10.1111/j.1365-2990.2011.01222.x
Gain of chromosome arm 1q in atypical meningioma correlates with shorter progression-free survival
Abstract
Aims: Atypical (World Health Organization grade II) meningiomas have moderately high recurrence rates; even for completely resected tumours, approximately one-third will recur. Post-operative radiotherapy may aid local control and improve survival, but carries the risk of side effects. More accurate prediction of recurrence risk is therefore needed for patients with atypical meningioma. Previously, we used high-resolution array comparative genomic hybridization to identify genetic variations in 47 primary atypical meningiomas and found that approximately 60% of tumours show gain of 1q at 1q25.1 and 1q25.3 to 1q32.1 and that 1q gain appeared to correlate with shorter progression-free survival. This study aimed to validate and extend these findings in an independent sample.
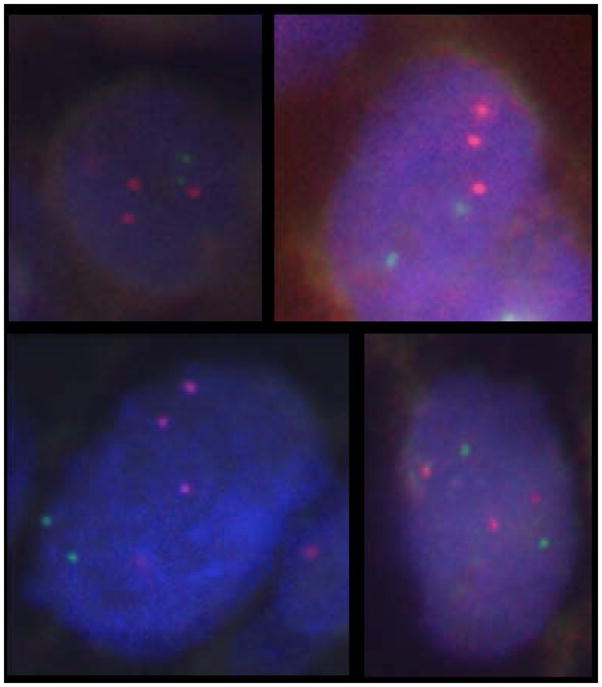
Methods: Eighty-six completely resected atypical meningiomas (with 25 recurrences) from two neurosurgical centres in Ireland were identified and clinical follow-up was obtained. Utilizing a dual-colour interphase fluorescence in situ hybridization assay, 1q gain was assessed using Bacterial Artificial Chromosome probes directed against 1q25.1 and 1q32.1.
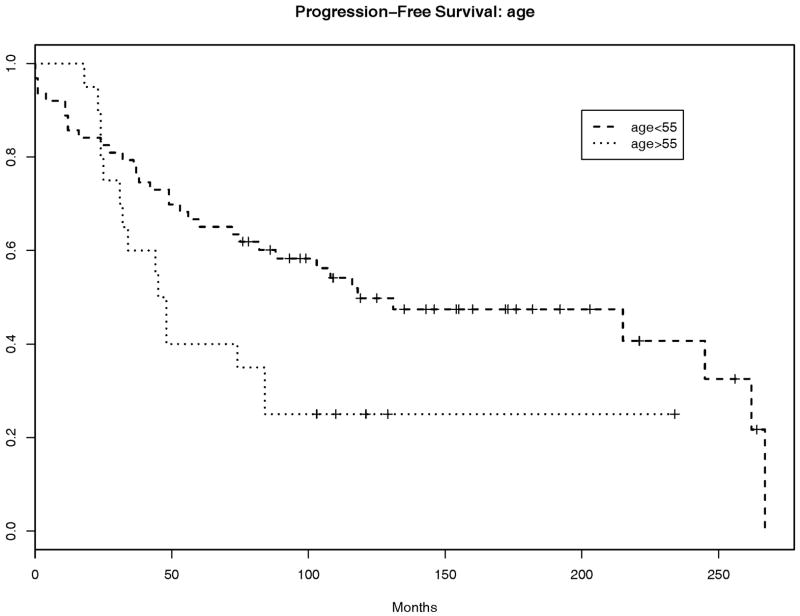
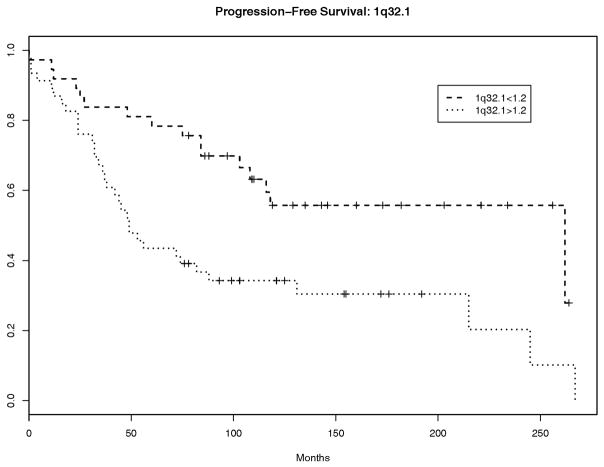
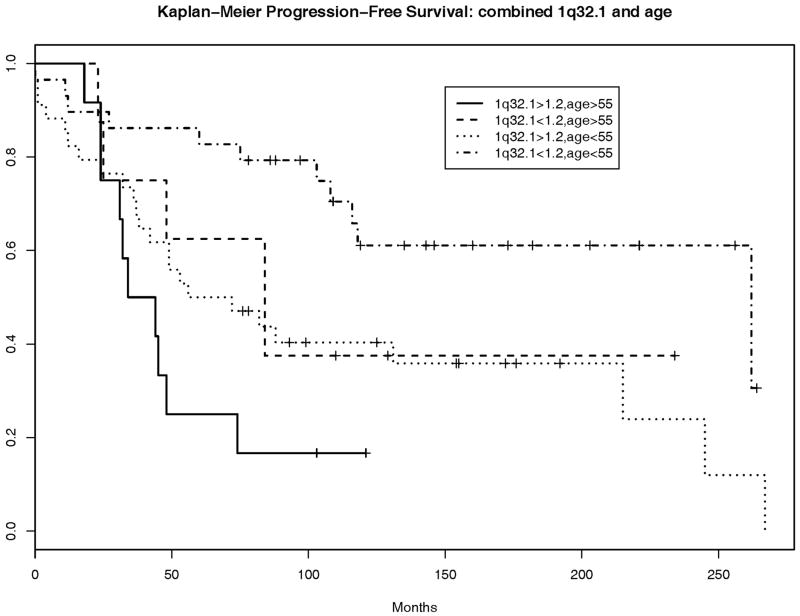
Results: The results confirm the high prevalence of 1q gain at these loci in atypical meningiomas. We further show that gain at 1q32.1 and age each correlate with progression-free survival in patients who have undergone complete surgical resection of atypical meningiomas.
Conclusions: These independent findings suggest that assessment of 1q copy number status can add clinically useful information for the management of patients with atypical meningiomas.
© 2011 The Authors. Neuropathology and Applied Neurobiology © 2011 British Neuropathological Society.
Conflict of interest statement
Conflicts of Interest
We declare that we have no conflicts of interest.
Figures
Similar articles
-
Early recurrences in histologically benign/grade I meningiomas are associated with large tumors and coexistence of monosomy 14 and del(1p36) in the ancestral tumor cell clone.Neuro Oncol. 2007 Oct;9(4):438-46. doi: 10.1215/15228517-2007-026. Epub 2007 Aug 17. Neuro Oncol. 2007. PMID: 17704362 Free PMC article.
-
Diagnostic and prognostic significance of genetic regional heterogeneity in meningiomas.Neuro Oncol. 2004 Oct;6(4):290-9. doi: 10.1215/S1152851704000158. Neuro Oncol. 2004. PMID: 15494096 Free PMC article.
-
Molecular biological determinations of meningioma progression and recurrence.PLoS One. 2014 Apr 10;9(4):e94987. doi: 10.1371/journal.pone.0094987. eCollection 2014. PLoS One. 2014. PMID: 24722350 Free PMC article.
-
Two cases of atypical meningioma with pulmonary metastases: a comparative cytogenetic analysis of chromosomes 1p and 22 and a review of the literature.Neuropathology. 2015 Apr;35(2):175-83. doi: 10.1111/neup.12177. Epub 2014 Nov 6. Neuropathology. 2015. PMID: 25376227 Review.
-
Atypical and malignant meningiomas: an outcome report of seventeen cases.J Neurooncol. 1998 Aug;39(1):65-70. doi: 10.1023/a:1005981731739. J Neurooncol. 1998. PMID: 9760071 Review.
Cited by
-
High Copy-Number Variation Burdens in Cranial Meningiomas From Patients With Diverse Clinical Phenotypes Characterized by Hot Genomic Structure Changes.Front Oncol. 2020 Aug 14;10:1382. doi: 10.3389/fonc.2020.01382. eCollection 2020. Front Oncol. 2020. PMID: 32923390 Free PMC article.
-
Prognostic significance of brain invasion in meningiomas: systematic review and meta-analysis.Brain Tumor Pathol. 2021 Apr;38(2):81-95. doi: 10.1007/s10014-020-00390-y. Epub 2021 Jan 6. Brain Tumor Pathol. 2021. PMID: 33403457
-
Estimation of the censoring distribution in clinical trials.Contemp Clin Trials Commun. 2021 Aug 30;23:100842. doi: 10.1016/j.conctc.2021.100842. eCollection 2021 Sep. Contemp Clin Trials Commun. 2021. PMID: 34504980 Free PMC article.
-
Integrated clinical genomic analysis reveals xenobiotic metabolic genes are downregulated in meningiomas of current smokers.J Neurooncol. 2023 Jun;163(2):397-405. doi: 10.1007/s11060-023-04359-7. Epub 2023 Jun 15. J Neurooncol. 2023. PMID: 37318677
-
Integrated molecular and detailed anatomical profiling identifies a prognostically adverse subtype of posterior fossa meningiomas: high-risk copy number alterations are associated with midline predilection and predict poor prognosis.Acta Neuropathol Commun. 2025 Aug 7;13(1):168. doi: 10.1186/s40478-025-02083-z. Acta Neuropathol Commun. 2025. PMID: 40775657 Free PMC article.
References
-
- Riemenschneider MJ, Perry A, Reifenberger G. Histological classification and molecular genetics of meningiomas. Lancet Neurol. 2006 Dec;5(12):1045–54. - PubMed
-
- Perry A, Scheithauer BW, Stafford SL, Lohse CM, Wollan PC. “Malignancy” in meningiomas: a clinicopathologic study of 116 patients, with grading implications. Cancer. 1999 May 1;85(9):2046–56. - PubMed
-
- Louis DN, Budka H. Meningiomas. In: Kleihues P, editor. World Health Organization classification of tumours; pathology and genetics of tumours of the central nervous system. Lyon: IARC Press; 2000. pp. 176–84.
-
- Perry A, Scheithauer BW, Budka H, von Deimling A. Meningeal tumours. In: Louis DN, Wiestler OD, Cavanee WK, editors. WHO classification of tumours of the central nervous system. Lyon: IARC; 2007. pp. 164–72.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
