

Prevalence and predictors of interval colorectal cancers in medicare beneficiaries
- PMID: 21989586
- PMCID: PMC3258472
- DOI: 10.1002/cncr.26602
Prevalence and predictors of interval colorectal cancers in medicare beneficiaries
Abstract
Background: After a colonoscopy that is negative for cancer, a subset of patients may be diagnosed with colorectal cancer, also termed interval cancer. The frequency and predictors have not been well studied in a population-based US cohort.
Methods: The authors used the linked Surveillance, Epidemiology, and End Results (SEER)-Medicare database to identify 57,839 patients aged ≥ 69 years who were diagnosed with colorectal cancer between 1994 and 2005 and who underwent colonoscopy within 6 months of cancer diagnosis. Colonoscopy performed between 6 and 36 months before cancer diagnosis was a proxy for interval cancer.
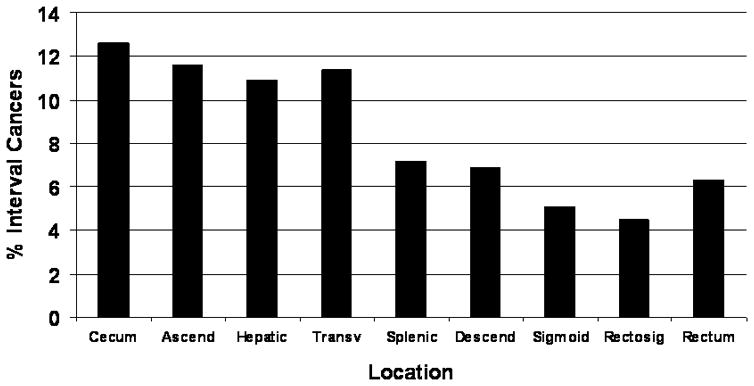
Results: By using the case definition, 7.2% of patients developed interval cancers. Factors that were associated with interval cancers included proximal tumor location (distal colon: multivariable odds ratio [OR], 0.42; 95% confidence interval [CI], 0.390-0.46; rectum: OR, 0.47; 95% CI, 0.42-0.53), increased comorbidity (OR, 1.89; 95% CI, 1.68 2.14 for ≥ 3 comorbidities), a previous diagnosis of diverticulosis (OR, 6.00; 95% CI, 5.57-6.46), and prior polypectomy (OR, 1.74; 95% CI, 1.62-1.87). Risk factors at the endoscopist level included a lower polypectomy rate (OR, 0.70; 95% CI, 0.63-0.78 for the highest quartile), higher colonoscopy volume (OR, 1.27; 95% CI, 1.13-1.43), and specialty other than gastroenterology (colorectal surgery: OR, 1.45; 95% CI, 1.16-1.83; general surgery: OR, 1.42; 95% CI, 1.24-1.62; internal medicine: OR, 1.38; 95% CI, 1.17-1.63; family practice: OR, 1.16; 95% CI, 1.00-1.35).
Conclusions: A significant proportion of patients developed interval colorectal cancer, particularly in the proximal colon. Contributing factors likely included both procedural and biologic factors, emphasizing the importance of meticulous examination of the mucosa.
Copyright © 2011 American Cancer Society.
Figures
References
-
- Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008. CA Cancer J Clin. 2008;58:130–60. - PubMed
-
- U S. Preventive Services Task Force. Screening for colorectal cancer: recommendations and rationale. Ann Intern Med. 2002;137:129–31. - PubMed
-
- Rex DK, Johnson DA, Anderson JC, Schoenfeld PS, Burke CA, Inadomi JM. American College of Gastroenterology guidelines for colorectal cancer screening 2008. Am J Gastroenterol. 2009;104:739–50. - PubMed
-
- Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med. 1993;329:1977–81. - PubMed
-
- Atkin WS, Morson BC, Cuzick J. Long-term risk of colorectal cancer after excision of rectosigmoid adenomas. N Engl J Med. 1992;326:658–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
