

TP53 mutations in serous tubal intraepithelial carcinoma and concurrent pelvic high-grade serous carcinoma--evidence supporting the clonal relationship of the two lesions
- PMID: 21990067
- PMCID: PMC4782784
- DOI: 10.1002/path.3023
TP53 mutations in serous tubal intraepithelial carcinoma and concurrent pelvic high-grade serous carcinoma--evidence supporting the clonal relationship of the two lesions
Abstract
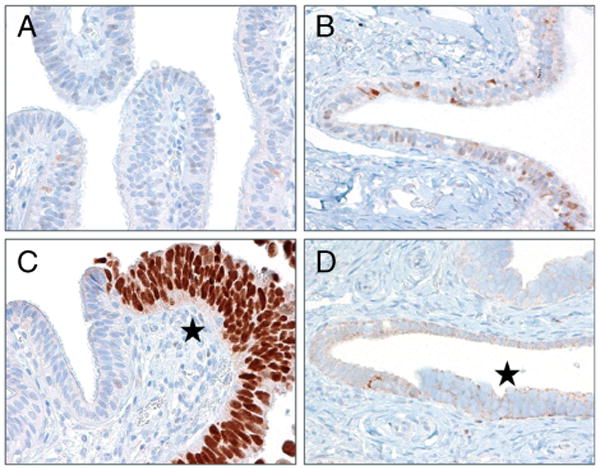
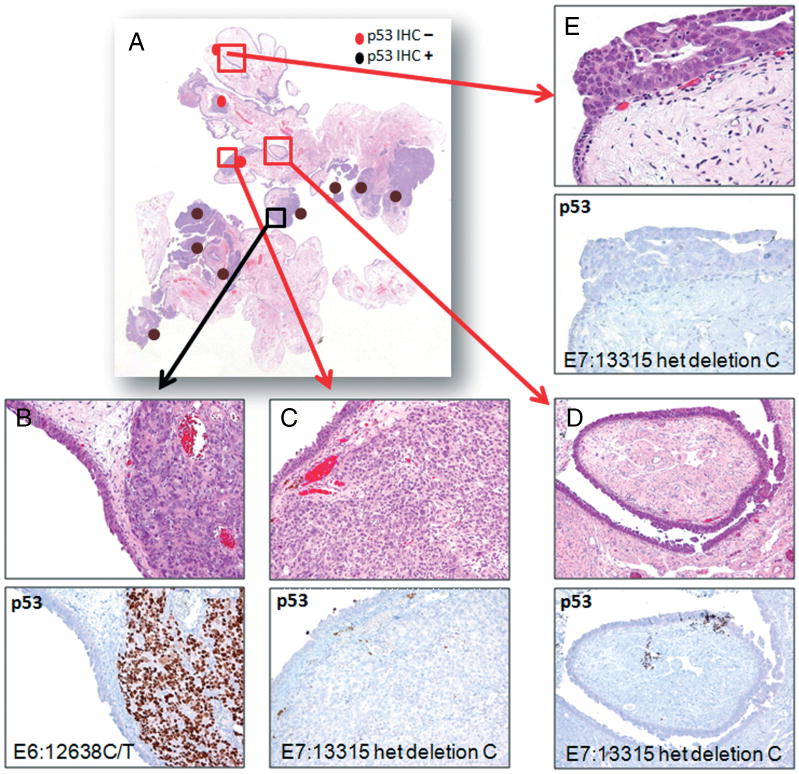
Serous tubal intraepithelial carcinomas (STICs) have been proposed to be the most likely precursor of ovarian, tubal and 'primary peritoneal' (pelvic) high-grade serous carcinoma (HGSC). As somatic mutation of TP53 is the most common molecular genetic change of ovarian HGSC, occurring in more than 95% of cases, we undertook a mutational analysis of 29 pelvic HGSCs that had concurrent STICs to demonstrate the clonal relationship of STICs and HGSCs. In addition, we correlated the mutational data with p53 immunostaining to determine the role of p53 immunoreactivity as a surrogate for TP53 mutations in histological diagnosis. Somatic TP53 mutations were detected in all 29 HGSCs analysed and the identical mutations were detected in 27 of 29 pairs of STICs and concurrent HGSCs. Missense mutations were observed in 61% of STICs and frameshift/splicing junction/nonsense mutations in 39%. Interestingly, there were two HGSCs with two distinctly different TP53 mutations each, but only one of the mutations was detected in the concurrent STICs. Missense mutations were associated with intense and diffuse (≥ 60%) p53 nuclear immunoreactivity, while most of the null mutations were associated with complete loss of p53 staining (p < 0.0001). Overall, this p53 staining pattern yielded a sensitivity of 87% and a specificity of 100% in detecting TP53 missense mutations. In conclusion, the above findings support the clonal relationship of STIC and pelvic HGSC and demonstrate the utility of p53 immunostaining as a surrogate for TP53 mutation in the histological diagnosis of STIC. In this regard, it is important to appreciate the significance of different staining patterns. Specifically, strong diffuse staining correlates with a missense mutation, whereas complete absence of staining correlates with null mutations.
Copyright © 2012 Pathological Society of Great Britain and Ireland. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
No conflicts of interest were declared.
Figures
References
-
- Callahan MJ, Crum CP, Medeiros F, et al. Primary Fallopian tube malignancies in BRCA-positive women undergoing surgery for ovarian cancer risk reduction. J Clin Oncol. 2007;25:3985–3990. - PubMed
-
- Przybycin CG, Kurman RJ, Ronnett BM, et al. Are all pelvic (nonuterine) serous carcinomas of tubal origin? Am J Surg Pathol. 2010;34:1407–1416. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
