

Fast Dixon whole-body MRI for detecting distant cancer metastasis: a preliminary clinical study
- PMID: 21990095
- PMCID: PMC3265627
- DOI: 10.1002/jmri.22815
Fast Dixon whole-body MRI for detecting distant cancer metastasis: a preliminary clinical study
Abstract
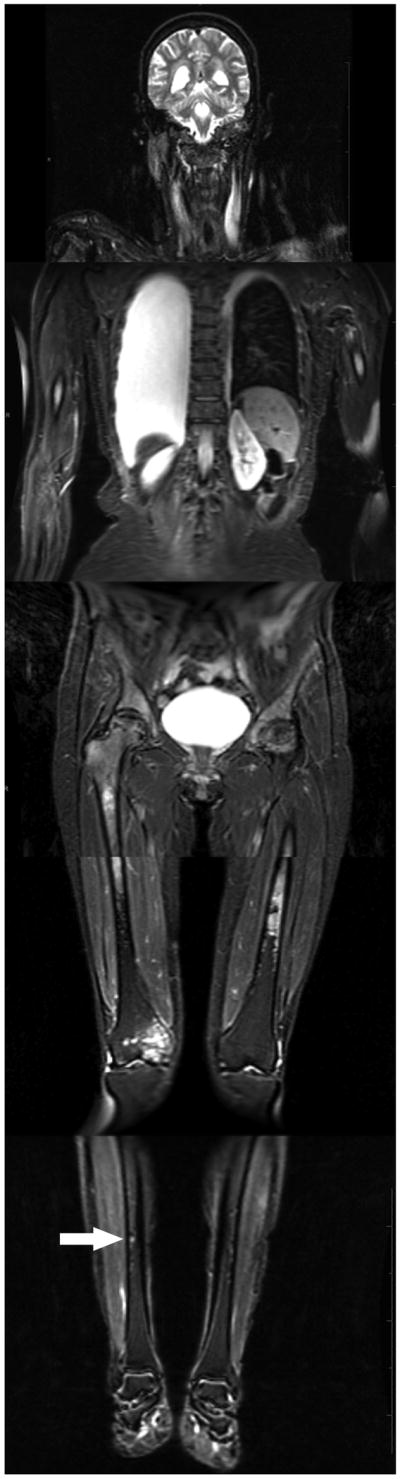
Purpose: To evaluate the feasibility of fast Dixon whole-body (WB) magnetic resonance imaging (MRI) for detecting bone and liver metastasis in clinical patients and to compare its performance with skeletal scintigraphy (SS) for detecting bone metastases using reference imaging with >1 year follow-up as the gold standard.
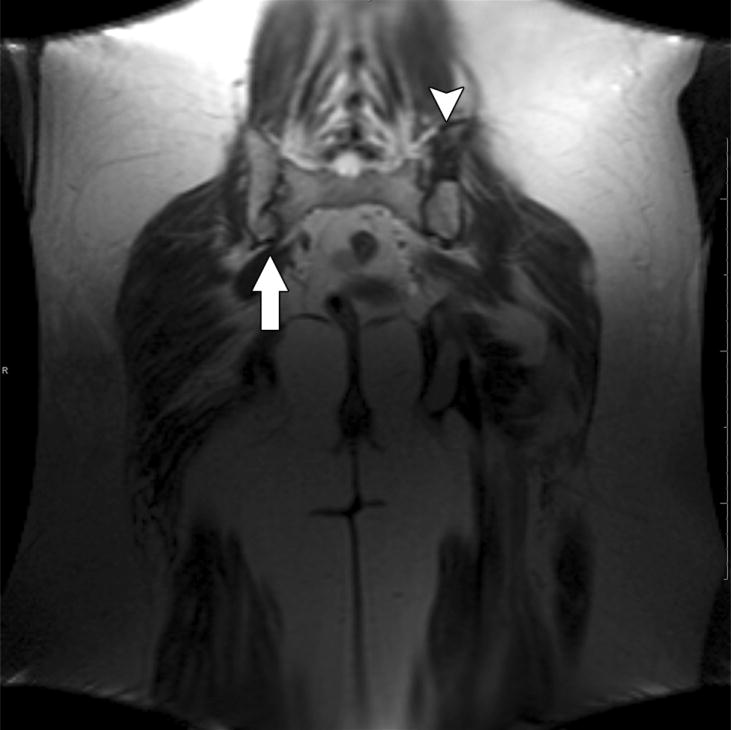
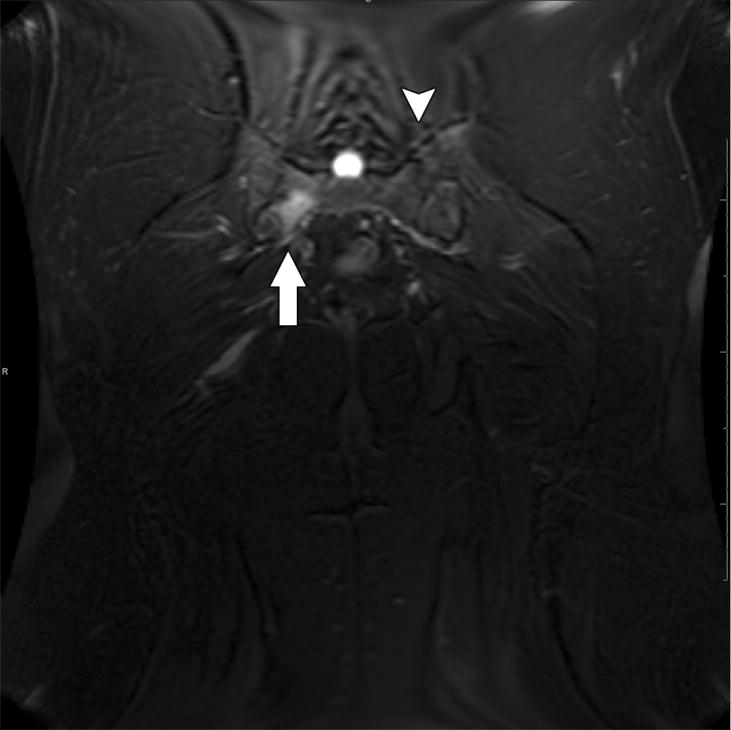
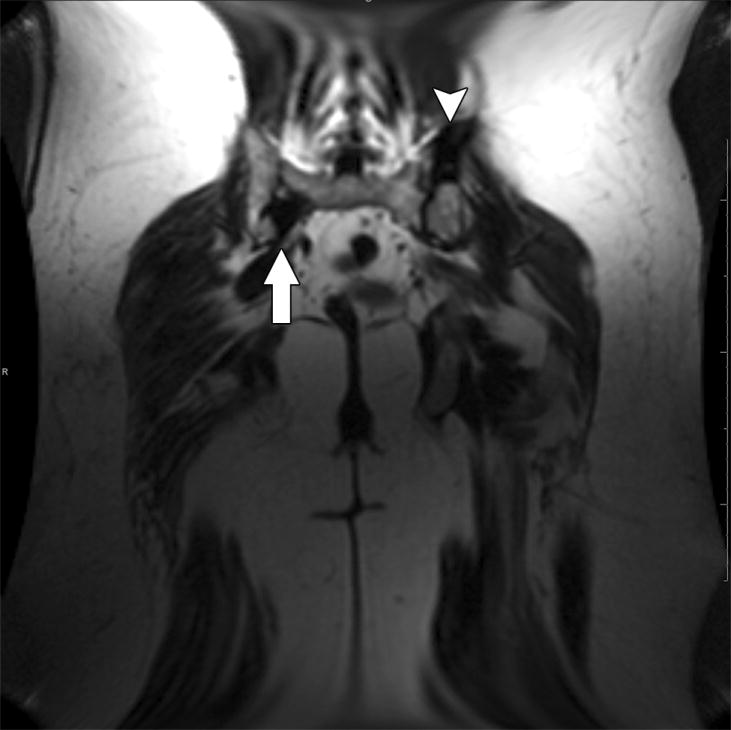
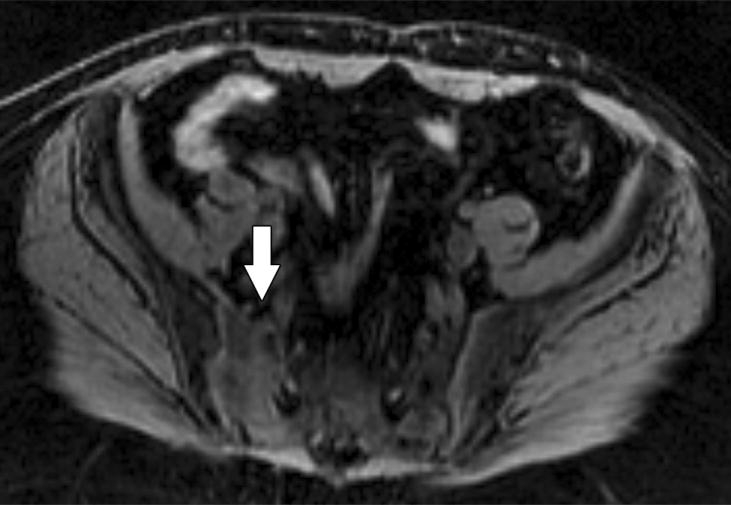
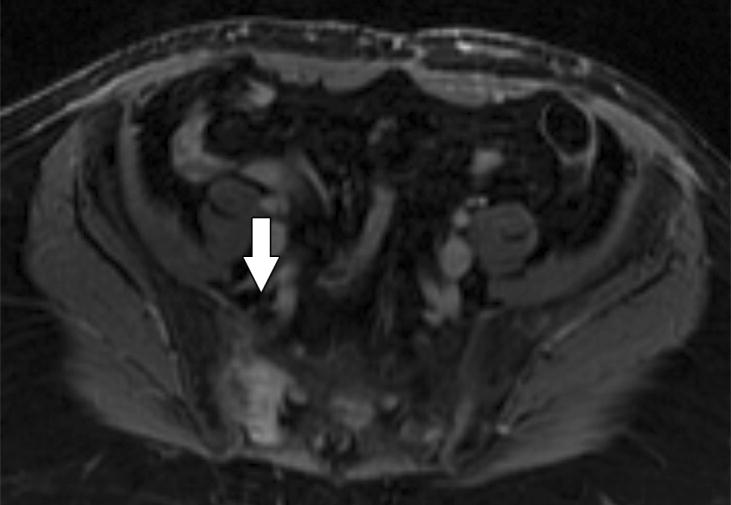
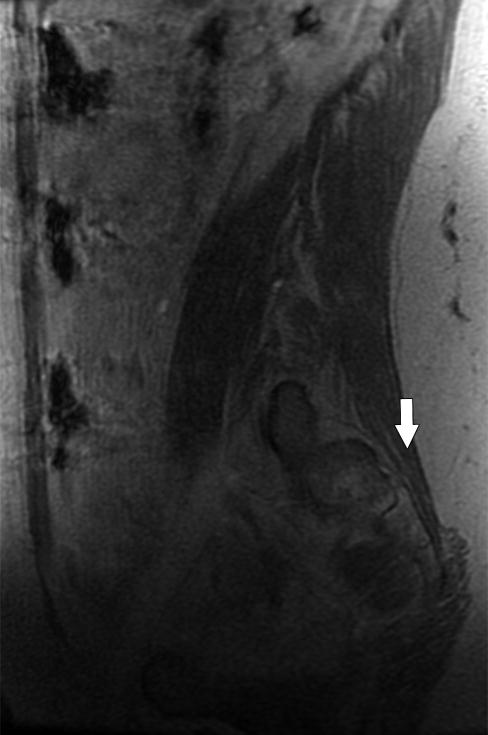
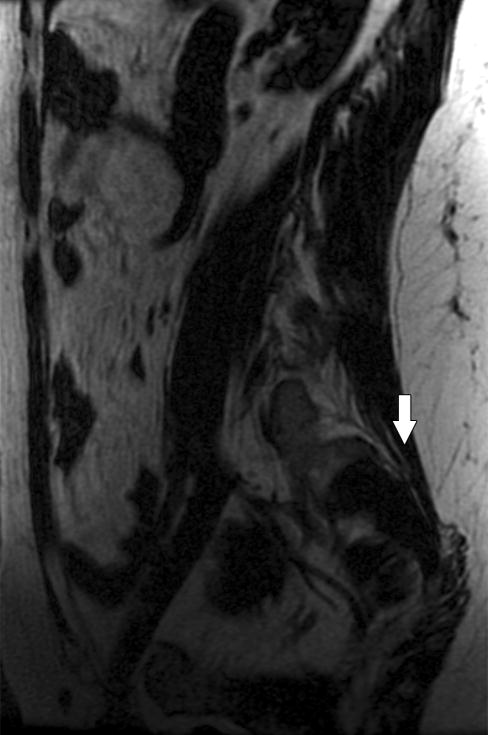
Materials and methods: Twenty-nine patients with bone metastases prospectively underwent WB MRI and SS. WB MRI included coronal T2, axial T1 with and without intravenous gadolinium (including triphasic liver sequences), and axial diffusion-weighted imaging, plus spinal sagittal postcontrast T1-weighted images. The skeleton was divided into 16 segments. Reviewers blinded to other images identified up to five lesions per segment and rated them using a five-point confidence scale for metastatic disease. Sensitivities and specificities were compared using the McNemar test.
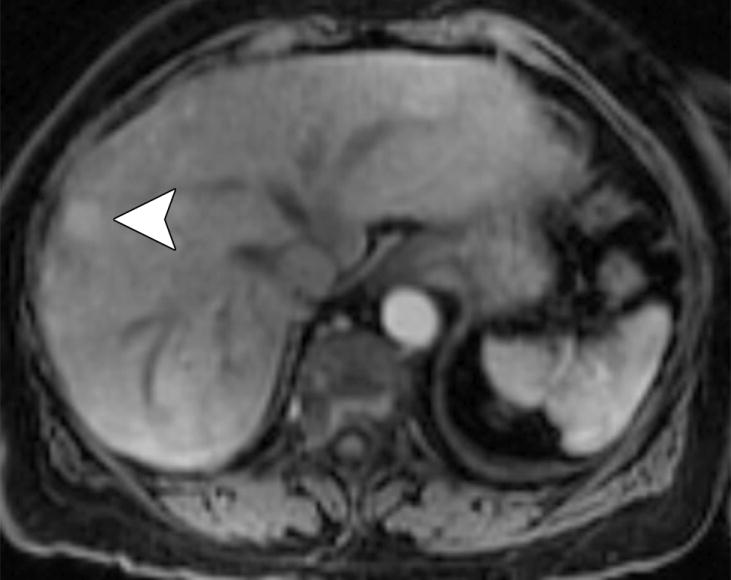
Results: The sensitivity of WB MRI and SS in detecting bone metastases was 70.8% and 59.6% (P = 0.003), respectively; specificity was 89.1% and 98.7% (P < 0.0001). WB MRI detected all livers with metastases (n = 8). One focal nodular hyperplasia was classified as a metastasis on WB MRI.
Conclusion: Fast Dixon WB MRI is feasible in clinical patients, highly specific, and more sensitive than SS in detecting bone metastases, and can detect metastases of the liver.
Copyright © 2011 Wiley Periodicals, Inc.
Conflict of interest statement
Figures













References
-
- Abrams HL, Spiro R, Goldstein N. Metastases in carcinoma; analysis of 1000 autopsied cases. Cancer. 1950;3:74–85. - PubMed
-
- Costelloe CM, Rohren EM, Madewell JE, et al. Imaging bone metastases in breast cancer: techniques and recommendations for diagnosis. Lancet Oncol. 2009;10:606–614. - PubMed
-
- Horvath LJ, Burtness BA, McCarthy S, Johnson KM. Total-body echo-planar MR imaging in the staging of breast cancer: comparison with conventional methods--early experience. Radiology. 1999;211:119–128. - PubMed
-
- Engelhard K, Hollenbach HP, Wohlfart K, von Imhoff E, Fellner FA. Comparison of whole-body MRI with automatic moving table technique and bone scintigraphy for screening for bone metastases in patients with breast cancer. Eur Radiol. 2004;14:99–105. - PubMed
-
- Lauenstein TC, Goehde SC, Herborn CU, et al. Whole-body MR imaging: evaluation of patients for metastases. Radiology. 2004;233:139–148. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
