

Cigarette smoke exposure induces CFTR internalization and insolubility, leading to airway surface liquid dehydration
- PMID: 21990373
- PMCID: PMC3290447
- DOI: 10.1096/fj.11-192377
Cigarette smoke exposure induces CFTR internalization and insolubility, leading to airway surface liquid dehydration
Abstract
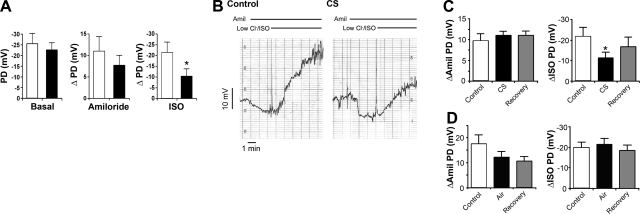
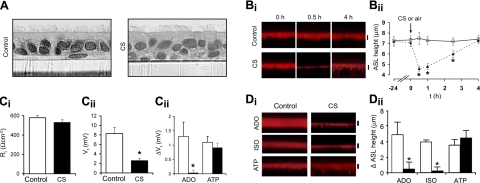
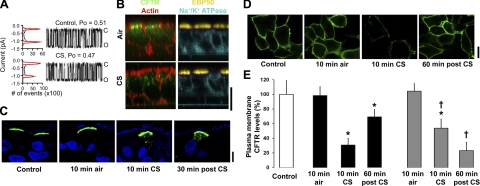
Cigarette smoke (CS) exposure induces mucus obstruction and the development of chronic bronchitis (CB). While many of these responses are determined genetically, little is known about the effects CS can exert on pulmonary epithelia at the protein level. We, therefore, tested the hypothesis that CS exerts direct effects on the CFTR protein, which could impair airway hydration, leading to the mucus stasis characteristic of both cystic fibrosis and CB. In vivo and in vitro studies demonstrated that CS rapidly decreased CFTR activity, leading to airway surface liquid (ASL) volume depletion (i.e., dehydration). Further studies revealed that CS induced internalization of CFTR. Surprisingly, CS-internalized CFTR did not colocalize with lysosomal proteins. Instead, the bulk of CFTR shifted to a detergent-resistant fraction within the cell and colocalized with the intermediate filament vimentin, suggesting that CS induced CFTR movement into an aggresome-like, perinuclear compartment. To test whether airway dehydration could be reversed, we used hypertonic saline (HS) as an osmolyte to rehydrate ASL. HS restored ASL height in CS-exposed, dehydrated airway cultures. Similarly, inhaled HS restored mucus transport and increased clearance in patients with CB. Thus, we propose that CS exposure rapidly impairs CFTR function by internalizing CFTR, leading to ASL dehydration, which promotes mucus stasis and a failure of mucus clearance, leaving smokers at risk for developing CB. Furthermore, our data suggest that strategies to rehydrate airway surfaces may provide a novel form of therapy for patients with CB.
Figures





References
-
- Mannino D. M., Homa D. M., Akinbami L. J., Ford E. S., Redd S. C. (2002) Chronic obstructive pulmonary disease surveillance–United States, 1971–2000. MMWR Surveill. Summ. 51, 1–16 - PubMed
-
- Gerald L. B., Bailey W. C. (2002) Global initiative for chronic obstructive lung disease. J. Cardiopulm. Rehabil. 22, 234–244 - PubMed
-
- Barnes P. J. (2004) Mediators of chronic obstructive pulmonary disease. Pharmacol. Rev. 56, 515–548 - PubMed
-
- Calverley P. M., Anderson J. A., Celli B., Ferguson G. T., Jenkins C., Jones P. W., Yates J. C., Vestbo J. (2007) Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N. Engl. J. Med. 356, 775–789 - PubMed
-
- Cantin A. M., Hanrahan J. W., Bilodeau G., Ellis L., Dupuis A., Liao J., Zielenski J., Durie P. (2006) Cystic fibrosis transmembrane conductance regulator function is suppressed in cigarette smokers. Am. J. Respir. Crit. Care. Med. 173, 1139–1144 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
