

Occult metastases in lymph nodes predict survival in resectable non-small-cell lung cancer: report of the ACOSOG Z0040 trial
- PMID: 21990404
- PMCID: PMC3221530
- DOI: 10.1200/JCO.2011.35.2500
Occult metastases in lymph nodes predict survival in resectable non-small-cell lung cancer: report of the ACOSOG Z0040 trial
Abstract
Purpose: The survival of patients with non-small-cell lung cancer (NSCLC), even when resectable, remains poor. Several small studies suggest that occult metastases (OMs) in pleura, bone marrow (BM), or lymph nodes (LNs) are present in early-stage NSCLC and are associated with a poor outcome. We investigated the prevalence of OMs in resectable NSCLC and their relationship with survival.
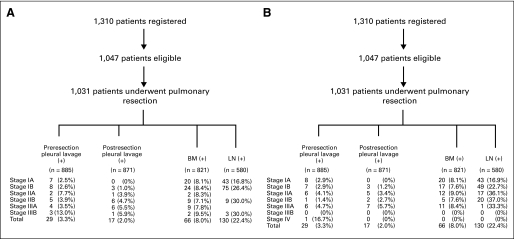
Patients and methods: Eligible patients had previously untreated, potentially resectable NSCLC. Saline lavage of the pleural space, performed before and after pulmonary resection, was examined cytologically. Rib BM and all histologically negative LNs (N0) were examined for OM, diagnosed by cytokeratin immunohistochemistry (IHC). Survival probabilities were estimated using the Kaplan-Meier method. The log-rank test and Cox proportional hazards regression model were used to compare survival of groups of patients. P < .05 was considered significant.
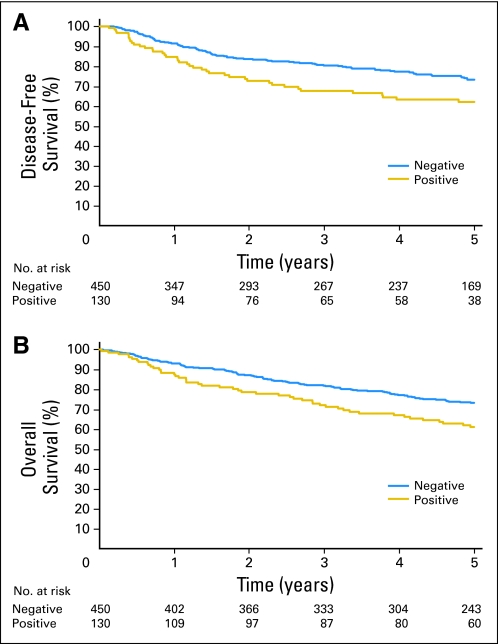
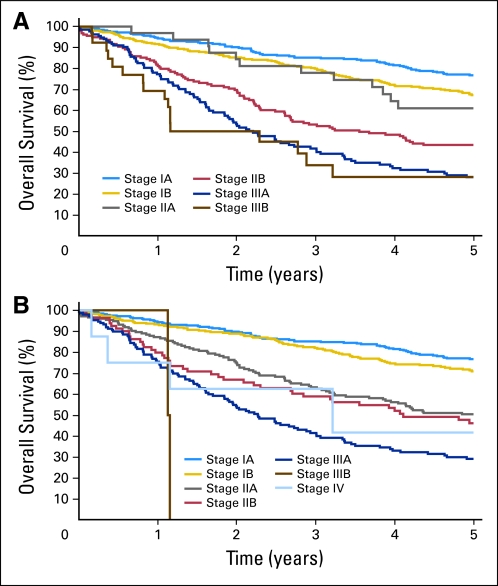
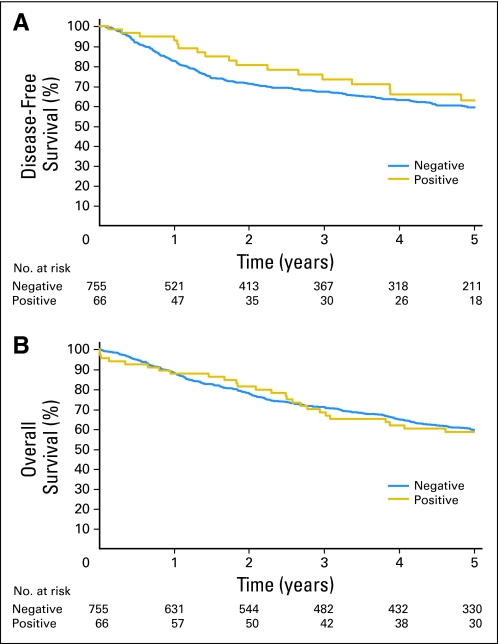
Results: From July 1999 to March 2004, 1,047 eligible patients (538 men and 509 women; median age, 67.2 years) were entered onto the study, of whom 50% had adenocarcinoma and 66% had stage I NSCLC. Pleural lavage was cytologically positive in only 29 patients. OMs were identified in 66 (8.0%) of 821 BM specimens and 130 (22.4%) of 580 LN specimens. In univariate and multivariable analyses OMs in LN but not BM were associated with significantly worse disease-free survival (hazard ratio [HR], 1.50; P = .031) and overall survival (HR, 1.58; P = .009).
Conclusion: In early-stage NSCLC, LN OMs detected by IHC identify patients with a worse prognosis. Future clinical trials should test the role of IHC in identifying patients for adjuvant therapy.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

Comment in
-
Occult nodal metastasis in non-small-cell lung cancer: implications for the radiation oncologist.J Clin Oncol. 2012 Jul 1;30(19):2423. doi: 10.1200/JCO.2011.41.2148. Epub 2012 May 21. J Clin Oncol. 2012. PMID: 22614992 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: Proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2:706–714. - PubMed
-
- Decker RH, Wilson LD. Postoperative radiation therapy for non-small cell lung cancer. Semin Thorac Cardiovasc Surg. 2008;20:184–187. - PubMed
-
- Wakelee H, Chhatwani L. Adjuvant chemotherapy for resected non-small cell lung cancer. Semin Thorac Cardiovasc Surg. 2008;20:198–203. - PubMed
-
- Price KAR, Azzoli CG, Gaspar LE. Chemoradiation for unresectable stage III non-small cell lung cancer. Semin Thorac Cardiovasc Surg. 2008;20:204–209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
