

Outcome prediction in pneumonia induced ALI/ARDS by clinical features and peptide patterns of BALF determined by mass spectrometry
- PMID: 21991318
- PMCID: PMC3184998
- DOI: 10.1371/journal.pone.0025544
Outcome prediction in pneumonia induced ALI/ARDS by clinical features and peptide patterns of BALF determined by mass spectrometry
Abstract
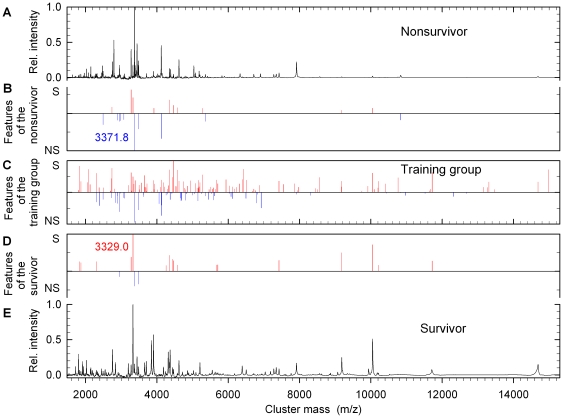
Background: Peptide patterns of bronchoalveolar lavage fluid (BALF) were assumed to reflect the complex pathology of acute lung injury (ALI)/acute respiratory distress syndrome (ARDS) better than clinical and inflammatory parameters and may be superior for outcome prediction.
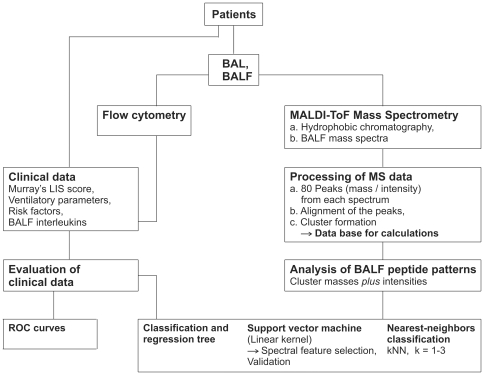
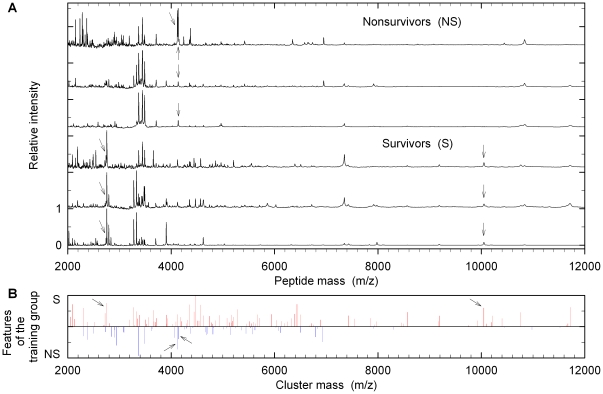
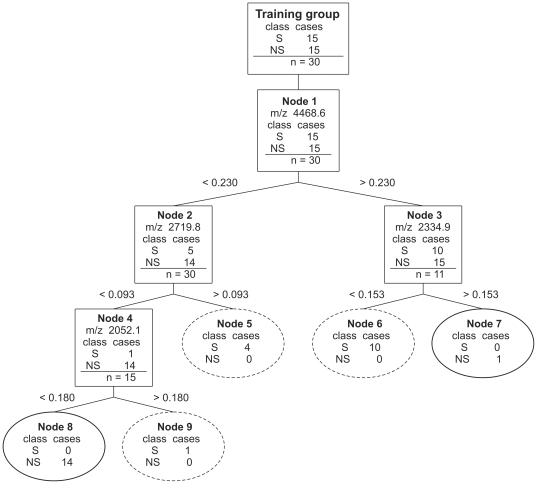
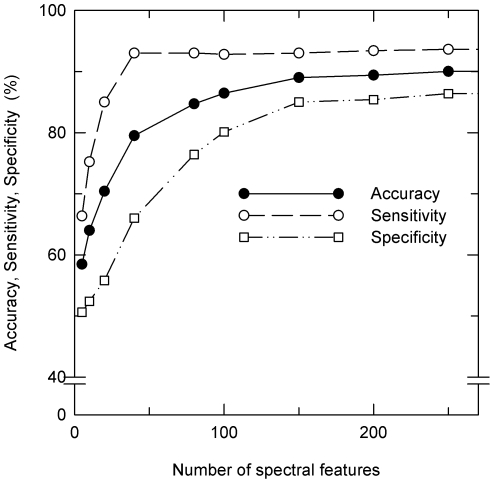
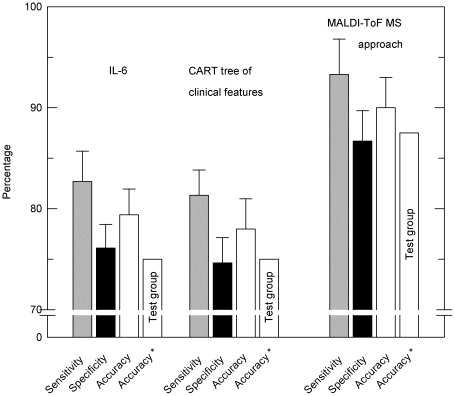
Methodology/principal findings: A training group of patients suffering from ALI/ARDS was compiled from equal numbers of survivors and nonsurvivors. Clinical history, ventilation parameters, Murray's lung injury severity score (Murray's LISS) and interleukins in BALF were gathered. In addition, samples of bronchoalveolar lavage fluid were analyzed by means of hydrophobic chromatography and MALDI-ToF mass spectrometry (MALDI-ToF MS). Receiver operating characteristic (ROC) analysis for each clinical and cytokine parameter revealed interleukin-6>interleukin-8>diabetes mellitus>Murray's LISS as the best outcome predictors. Outcome predicted on the basis of BALF levels of interleukin-6 resulted in 79.4% accuracy, 82.7% sensitivity and 76.1% specificity (area under the ROC curve, AUC, 0.853). Both clinical parameters and cytokines as well as peptide patterns determined by MALDI-ToF MS were analyzed by classification and regression tree (CART) analysis and support vector machine (SVM) algorithms. CART analysis including Murray's LISS, interleukin-6 and interleukin-8 in combination was correct in 78.0%. MALDI-ToF MS of BALF peptides did not reveal a single identifiable biomarker for ARDS. However, classification of patients was successfully achieved based on the entire peptide pattern analyzed using SVM. This method resulted in 90% accuracy, 93.3% sensitivity and 86.7% specificity following a 10-fold cross validation (AUC = 0.953). Subsequent validation of the optimized SVM algorithm with a test group of patients with unknown prognosis yielded 87.5% accuracy, 83.3% sensitivity and 90.0% specificity.
Conclusions/significance: MALDI-ToF MS peptide patterns of BALF, evaluated by appropriate mathematical methods can be of value in predicting outcome in pneumonia induced ALI/ARDS.
Conflict of interest statement
Figures

Similar articles
-
[Early diagnostic and prognosis prediction of circ_0054633 for acute lung injury/acute respiratory distress syndrome in children with severe pneumonia].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Sep;36(9):957-961. doi: 10.3760/cma.j.cn121430-20240506-00403. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 39380517 Chinese.
-
Comparative analysis of the alveolar macrophage proteome in ALI/ARDS patients between the exudative phase and recovery phase.BMC Immunol. 2013 Jun 17;14:25. doi: 10.1186/1471-2172-14-25. BMC Immunol. 2013. PMID: 23773529 Free PMC article.
-
The role of procalcitonin and IL-6 in discriminating between septic and non-septic causes of ALI/ARDS: a prospective observational study.Clin Chem Lab Med. 2013 Jul;51(7):1535-42. doi: 10.1515/cclm-2012-0562. Clin Chem Lab Med. 2013. PMID: 23314554
-
Performance of matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF-MS) in diagnosis of ovarian cancer: a systematic review and meta-analysis.J Ovarian Res. 2020 Jan 10;13(1):6. doi: 10.1186/s13048-019-0605-2. J Ovarian Res. 2020. PMID: 31924227 Free PMC article.
-
Interesting effects of interleukins and immune cells on acute respiratory distress syndrome.Clin Exp Med. 2023 Nov;23(7):2979-2996. doi: 10.1007/s10238-023-01118-w. Epub 2023 Jun 18. Clin Exp Med. 2023. PMID: 37330918 Review.
Cited by
-
The aging lung: microenvironment, mechanisms, and diseases.Front Immunol. 2024 May 2;15:1383503. doi: 10.3389/fimmu.2024.1383503. eCollection 2024. Front Immunol. 2024. PMID: 38756780 Free PMC article. Review.
-
Lung fluid biomarkers for acute respiratory distress syndrome: a systematic review and meta-analysis.Crit Care. 2019 Feb 12;23(1):43. doi: 10.1186/s13054-019-2336-6. Crit Care. 2019. PMID: 30755248 Free PMC article.
-
Galloyl-Hexahydroxydiphenoyl (HHDP)-Glucose Isolated From Punica granatum L. Leaves Protects Against Lipopolysaccharide (LPS)-Induced Acute Lung Injury in BALB/c Mice.Front Immunol. 2019 Aug 20;10:1978. doi: 10.3389/fimmu.2019.01978. eCollection 2019. Front Immunol. 2019. PMID: 31481965 Free PMC article.
-
Role of autophagy in lung diseases and ageing.Eur Respir Rev. 2022 Dec 21;31(166):220134. doi: 10.1183/16000617.0134-2022. Print 2022 Dec 31. Eur Respir Rev. 2022. PMID: 36543345 Free PMC article. Review.
-
The top 2,000 cited articles in critical care medicine: a bibliometric analysis.J Thorac Dis. 2018 Apr;10(4):2437-2447. doi: 10.21037/jtd.2018.03.178. J Thorac Dis. 2018. PMID: 29850150 Free PMC article.
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. New Engl J Med. 2000;342:1334–1349. - PubMed
-
- Ware LB. Prognostic determinants of acute respiratory distress syndrome in adults: impact on clinical trial design. Crit Care Med. 2005;33(3) Suppl:S217–S222. - PubMed
-
- Rubenfeld GD, Herridge MS. Epidemiology and outcomes of acute lung injury. Chest. 2007;131:554–562. - PubMed
-
- Zambon M, Vincent JL. Mortality rates for patients with acute lung injury/ARDS have decreased over time. Chest. 2008;133:1120–1127. - PubMed
-
- Girard TD, Bernard GR. Mechanical ventilation in ARDS: a state-of-the-art review. Chest. 2007;131:921–929. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
