

The use of structural allograft in primary and revision knee arthroplasty with bone loss
- PMID: 21991418
- PMCID: PMC3180775
- DOI: 10.4061/2011/578952
The use of structural allograft in primary and revision knee arthroplasty with bone loss
Abstract
Bone loss around the knee in the setting of total knee arthroplasty remains a difficult and challenging problem for orthopaedic surgeons. There are a number of options for dealing with smaller and contained bone loss; however, massive segmental bone loss has fewer options. Small, contained defects can be treated with cement, morselized autograft/allograft or metal augments. Segmental bone loss cannot be dealt with through simple addition of cement, morselized autograft/allograft, or metal augments. For younger or higher demand patients, the use of allograft is a good option as it provides a durable construct with high rates of union while restoring bone stock for future revisions. Older patients, or those who are low demand, may be better candidates for a tumour prosthesis, which provides immediate ability to weight bear and mobilize.
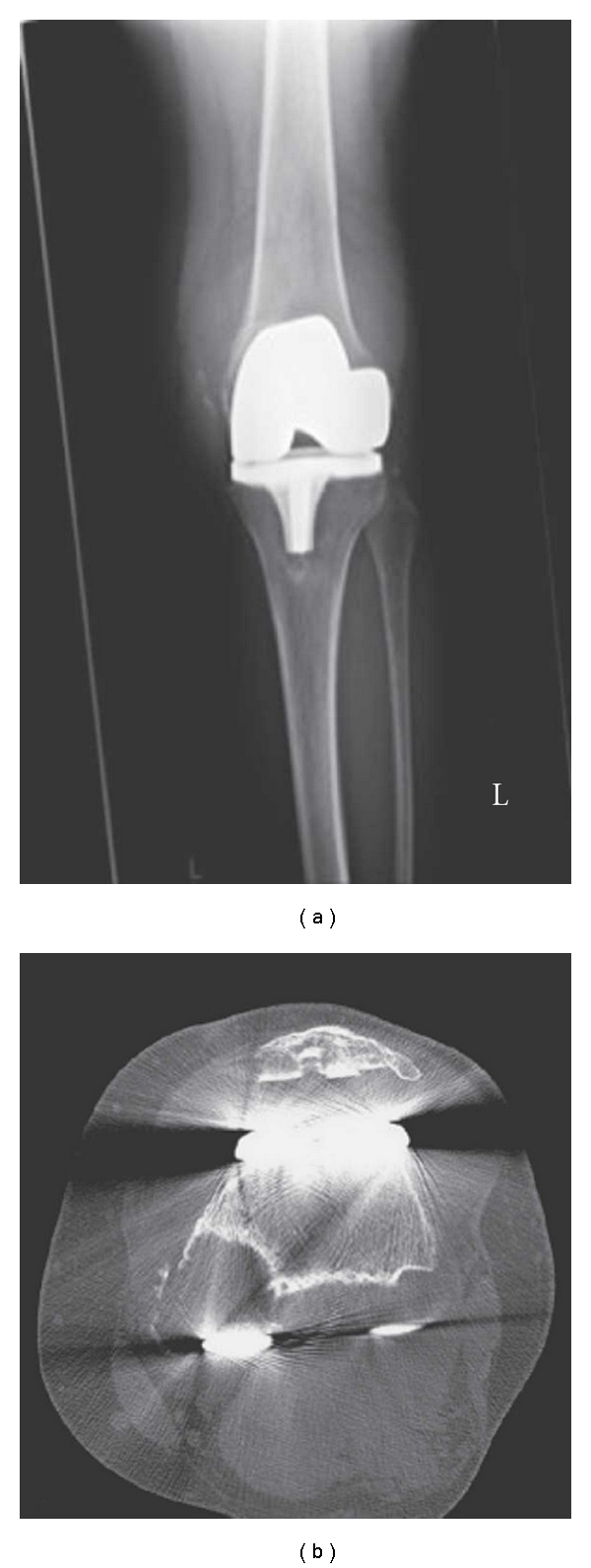
Figures



References
-
- Engh GA. Bone defect classification. In: Engh GA, Rorabeck CH, editors. Revision Total Knee Arthroplasty. Baltimore, Md, USA: Lippincott Williams & Wilkins; 1997. pp. 63–120.
-
- Backstein D, Safir O, Gross A. Management of bone loss: structural grafts in revision total knee arthroplasty. Clinical Orthopaedics and Related Research. 2006;(446):104–112. - PubMed
-
- Gross AE, Aubin P, Cheah HK, Davis AM, Ghazavi MT. A fresh osteochondral allograft alternative. Journal of Arthroplasty. 2002;17(4, supplement 1):50–53. - PubMed
-
- Gross AE, McKee NH, Pritzker KPH, Langer F. Reconstruction of skeletal deficits at the knee: a comprehensive osteochondral transplant program. Clinical Orthopaedics and Related Research. 1983;174:96–106. - PubMed
LinkOut - more resources
Full Text Sources
