

Anesthetic Routines: The Anesthesiologist's Role in GI Recovery and Postoperative Ileus
- PMID: 21991449
- PMCID: PMC3168940
- DOI: 10.4061/2011/976904
Anesthetic Routines: The Anesthesiologist's Role in GI Recovery and Postoperative Ileus
Abstract
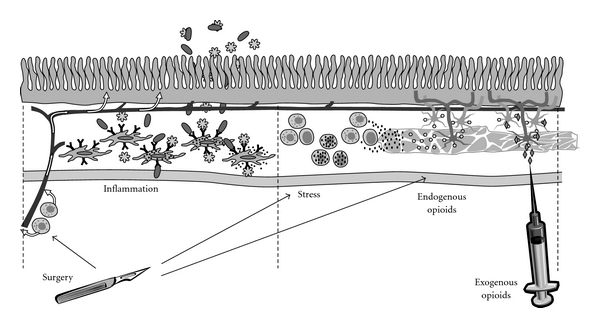
All patients undergoing bowel resection experience postoperative ileus, a transient cessation of bowel motility that prevents effective transit of intestinal contents or tolerance of oral intake, to varying degrees. An anesthesiologist plays a critical role, not only in the initiation of surgical anesthesia, but also with the selection and transition to effective postoperative analgesia regimens. Attempts to reduce the duration of postoperative ileus have prompted the study of various preoperative, perioperative, and postoperative regimens to facilitate gastrointestinal recovery. These include modifiable variables such as epidural anesthesia and analgesia, opioid-sparing anesthesia and analgesia, fluid restriction, colloid versus crystalloid combinations, prokinetic drugs, and use of the new peripherally acting mu-opioid receptor (PAM-OR) antagonists. Review and appropriate adaptation of these multiple modifiable interventions by anesthesiologists and their surgical colleagues will facilitate implementation of a best-practice management routine for bowel resection procedures that will benefit the patient and the healthcare system.
Figures
References
-
- Delaney CP. Clinical perspective on postoperative ileus and the effect of opiates. Neurogastroenterology and Motility. 2004;16(2):61–66. - PubMed
-
- Livingston EH, Passaro EP. Postoperative ileus. Digestive Diseases and Sciences. 1990;35(1):121–132. - PubMed
-
- Boeckxstaens GE, de Jonge WJ. Neuroimmune mechanisms in postoperative ileus. Gut. 2009;58(9):1300–1311. - PubMed
-
- Kehlet H, Holte K. Review of postoperative ileus. American Journal of Surgery. 2001;182(5):3S–10S. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
