

Long-term followup with evaluation of the surgical and functional results of the ileal pouch reservoir in restorative proctocolectomy for ulcerative colitis
- PMID: 21991523
- PMCID: PMC3168493
- DOI: 10.5402/2011/625842
Long-term followup with evaluation of the surgical and functional results of the ileal pouch reservoir in restorative proctocolectomy for ulcerative colitis
Abstract
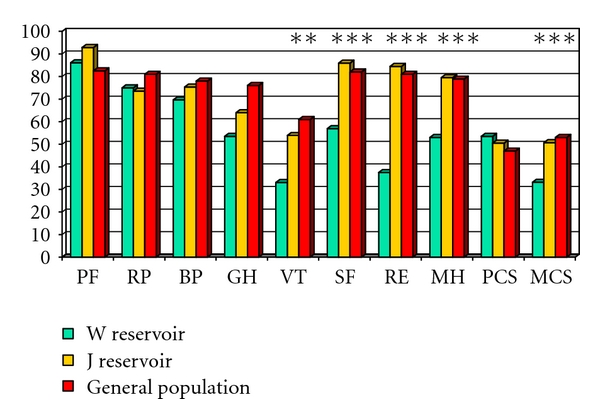
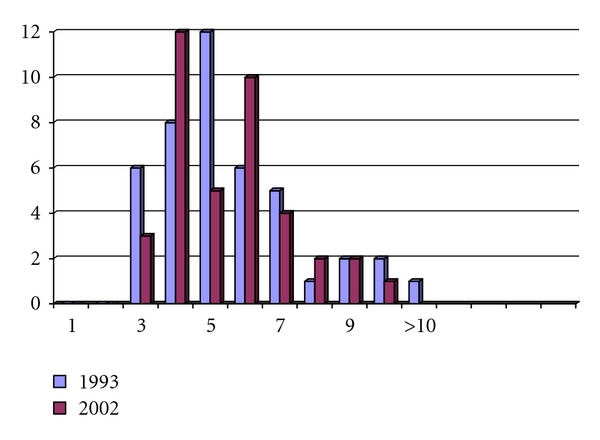
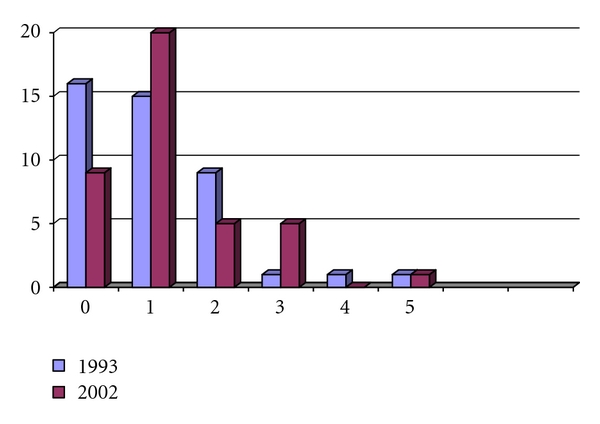
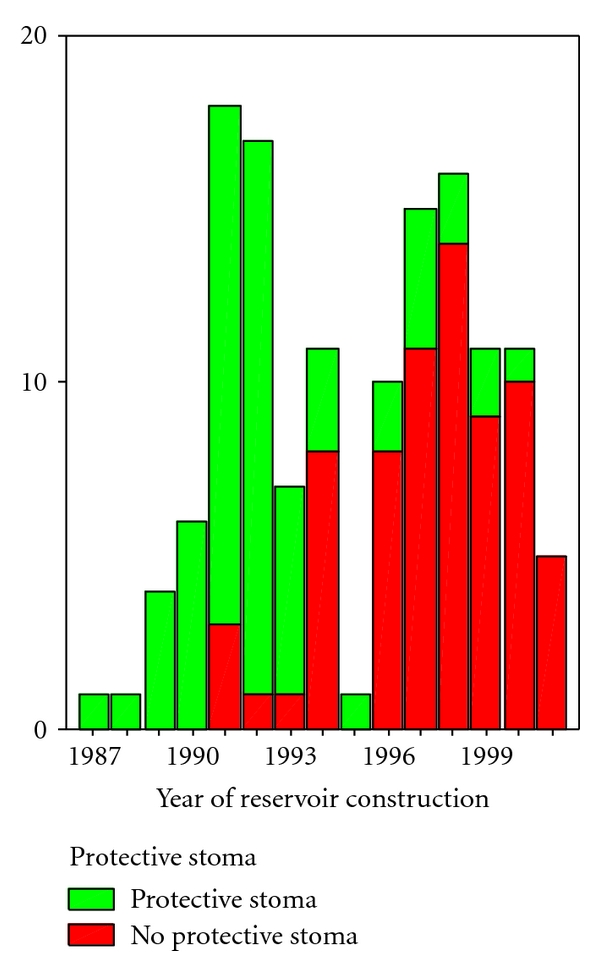
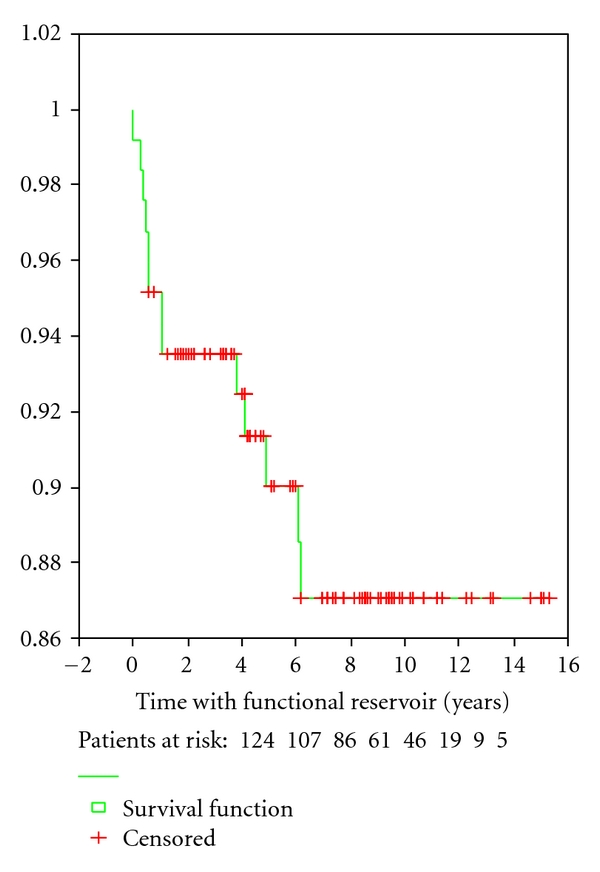
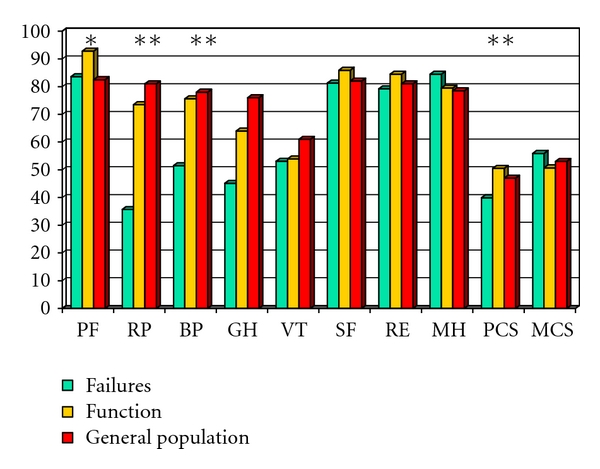
Aims. Evaluate the early and long term surgical and functional results of the ileal pouch-reservoir (IPAA) in patients with intractable ulcerative colitis. Material and Methods. Followup of 134 consecutive patients with W-or J-ileal pouch by diseases-specific and general health (SF-36) questionnaire. In the first 44 patients, early and late followup was performed. Results. Followup was performed 7.4 years (0.5-17 years) after construction of W (n = 9) and J (n = 125) ileal pouch, which had similar results. There were 14.9% early and 43.6% late complications with 12.7% early and 19.5% late reoperations. Protecting loop-ileostomy used in 54 patients (43.9%), did not protect against complications. Thirteen reservoirs (9.8%) were resected (n = 8) or deactivated (n = 5) due to functional failure. Operation time, postoperative complications and pouchitis were determinators for reservoir failure and reduced quality of life. The functional results at followup of 44 patients at 2.5 years (0.8-6.7 years) and 11.5 years (8.2-19.2 years) were remarkably similar. Conclusions. IPAA is a good option for most patients when medication fails. 10% experience failure with inferior quality of life. Protective stoma will not reduce failure rates. After an initial time period, reservoir function will not change over time.
Figures
References
-
- Corman ML, editor. Colon & Rectal Surgery. Philadelphia, Pa, USA: Lippincott Williams & Wilkins; 2005.
-
- McIntyre PB, Pemberton JH, Wolff BG, Dozois RR, Beart RW. Indeterminate colitis: long-term outcome in patients after ileal pouch-anal anastomosis. Diseases of the Colon and Rectum. 1995;38(1):51–54. - PubMed
-
- Yu CS, Pemberton JH, Larson D. Ileal pouch-anal anastomosis in patients with indeterminate colitis. Long-term results. Diseases of the Colon and Rectum. 2000;43(11):1487–1496. - PubMed
LinkOut - more resources
Full Text Sources
