

Surgical procedures in the treatment of 784 infected THAs reported to the Norwegian Arthroplasty Register
- PMID: 21992085
- PMCID: PMC3242948
- DOI: 10.3109/17453674.2011.623572
Surgical procedures in the treatment of 784 infected THAs reported to the Norwegian Arthroplasty Register
Abstract
Background and purpose: Controversies still exist regarding the best surgical procedure in the treatment of periprosthetic infection after total hip arthroplasty (THA). Based on data in the Norwegian Arthroplasty Register (NAR), we have compared the risk of re-revision after 4 different surgical procedures: 2-stage with exchange of the whole prosthesis, 1-stage with exchange of the whole prosthesis, major partial 1-stage with exchange of stem or cup, and minor partial 1-stage with exchange of femoral head and/or acetabular liner.
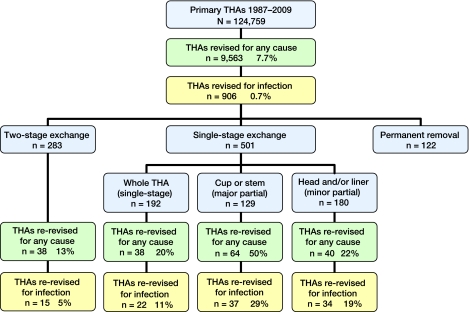
Methods: Between 1987 and 2009, 124,759 primary THAs were reported to the NAR, of which 906 (0.7%) were revised due to infection. Included in this study were the 784 revisions that had been performed by 1 of the 4 different surgical procedures. Cox-estimated survival and relative revision risks are presented with adjustment for differences among groups regarding gender, type of fixation, type of prosthesis, and age at revision.
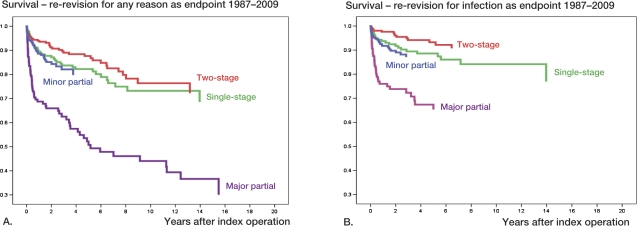
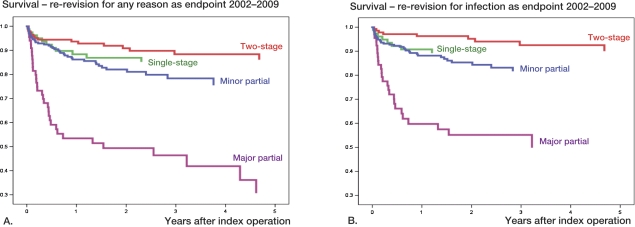
Results: 2-stage procedures were used in 283 revisions (36%), 1-stage in 192 revisions (25%), major partial in 129 revisions (17%), and minor partial in 180 revisions (23%). 2-year Kaplan-Meier survival for all revisions was 83%; it was 92% for those re-revised by 2-stage exchange procedure, 88% for those re-revised by 1-stage exchange procedure, 66% for those re-revised by major partial exchange procedure, and it was 76% for those re-revised by minor partial exchange. Compared to the 2-stage procedure and with any reason for revision as endpoint (180 re-revisions), the risk of re-revision increased 1.4 times for 1-stage (p = 0.2), 4.1 times for major partial exchange (p < 0.001), and 1.5 times for minor partial exchange (p = 0.1). With infection as the endpoint (108 re-revisions), the risk of re-revision increased 2.0 times for 1-stage exchange (p = 0.04), 6.0 times for major partial exchange (p < 0.001), and 2.3 times for minor partial exchange (p = 0.02). Similar results were found when the analyses were restricted to the period 2002-2009.
Interpretation: In the Norwegian Arthroplasty Register, the survival after revision of infected primary THA with 2-stage implant exchange was slightly superior to that for 1-stage exchange of the whole prosthesis. This result is noteworthy, since 2-stage procedures are often used with the most severe infections. However, debridement with exchange of head and/or liner but with retention of the fixed implant (minor revision) meant that there was a 76% chance of not being re-revised within 2 years.
Figures
References
-
- Azzam KA, Seeley M, Ghanem E, Austin MS, Purtill JJ, Parvizi J. Irrigation and debridement in the management of prosthetic joint infection: traditional indications revisited. J Arthroplasty. 2010;25(7):1022–7. - PubMed
-
- Biring GS, Kostamo T, Garbuz DS, Masri BA, Duncan CP. Two-stage revision arthroplasty of the hip for infection using an interim articulated Prostalac hip spacer: a 10- to 15-year follow-up study. J Bone Joint Surg (Br) 2009;91(11):1431–7. - PubMed
-
- Bozic KJ, Kurtz SM, Lau E, Ong K, Vail TP, Berry DJ. The epidemiology of revision total hip arthroplasty in the United States. J Bone Joint Surg (Am) 2009;91(1):128–33. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical