

Role of flow cytometry immunophenotyping in the diagnosis of leptomeningeal carcinomatosis
- PMID: 21993441
- PMCID: PMC3245993
- DOI: 10.1093/neuonc/nor172
Role of flow cytometry immunophenotyping in the diagnosis of leptomeningeal carcinomatosis
Abstract
Purpose: To explore the contribution of flow cytometry immunophenotyping (FCI) in detecting leptomeningeal disease in patients with solid tumors.
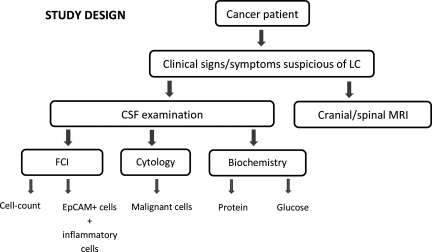
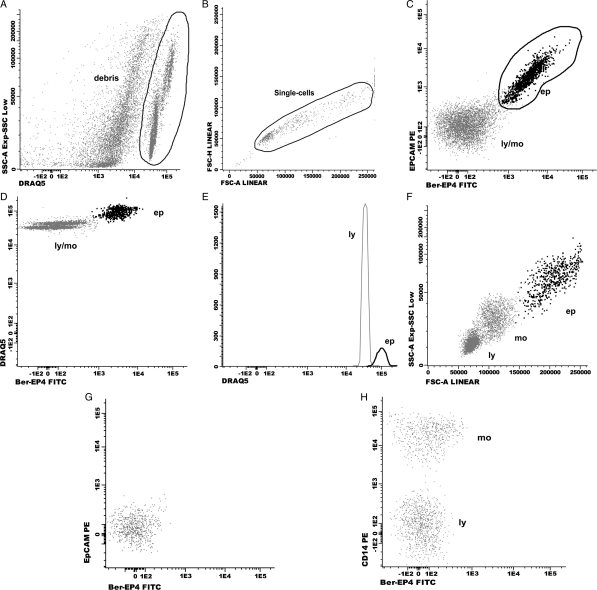
Experimental design: Cerebrospinal fluid (CSF) samples from 78 patients who received a diagnosis of epithelial-cell solid tumors and had clinical data suggestive of leptomeningeal carcinomatosis (LC) were studied. A novel FCI protocol was used to identify cells expressing the epithelial cell antigen EpCAM and their DNA content. Accompanying inflammatory cells were also described. FCI results (positive or negative for malignancy) were compared with those from CSF cytology and with the diagnosis established by the clinicians: patients with LC (n = 49), without LC (n = 26), and undetermined (n = 3).
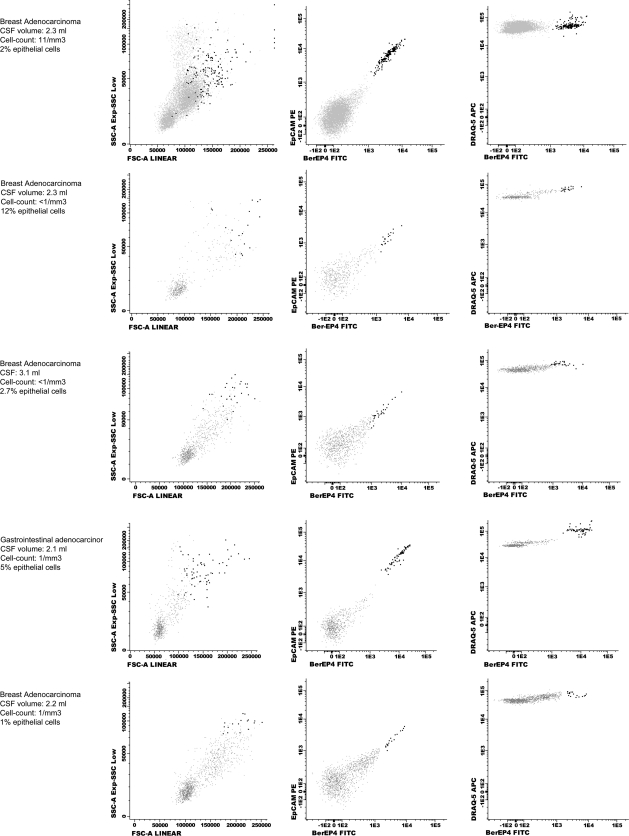
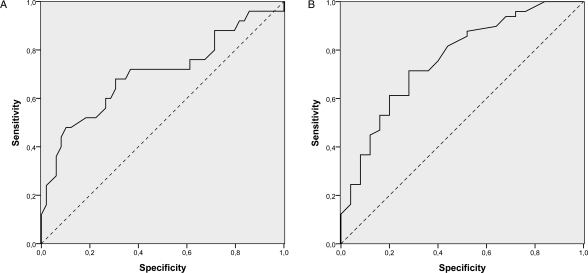
Results: FCI described a wide range of EpCAM-positive cells with a hyperdiploid DNA content in the CSF of patients with LC. Compared with cytology, FCI showed higher sensitivity (75.5 vs 65.3) and negative predictive value (67.6 vs 60.5), and similar specificity (96.1 vs 100) and positive predictive value (97.4 vs 100). Concordance between cytology and FCI was high (Kp = 0.83), although misdiagnosis of LC did not show differences between evaluating the CSF with 1 or 2 techniques (P = .06). Receiver-operator characteristic curve analyses showed that lymphocytes and monocytes had a different distribution between patients with and without LC.
Conclusion: FCI seems to be a promising new tool for improving the diagnostic examination of patients with suspicion of LC. Detection of epithelial cells with a higher DNA content is highly specific of LC, but evaluation of the nonepithelial cell compartment of the CSF might also be useful for supporting this diagnosis.
Figures
References
-
- Chamberlain MC, Glantz M, Groves MD, Wilson WH. Diagnostic tools for neoplastic meningitis: detecting disease, identifying patient risk, and determining benefit of treatment. Semin Oncol. 2009;36(4, Suppl 2):S35–S45. doi:10.1053/j.seminoncol.2009.05.005. - DOI - PubMed
-
- Gleissner B, Chamberlain MC. Neoplastic meningitis. Lancet Neurol. 2006;5(5):443–452. doi:10.1016/S1474-4422(06)70443-4. - DOI - PubMed
-
- Strik H, Prömmel P. Neoplastic meningitis. Diagnosis and individualized therapy. Expert Rev Anticancer Ther. 2010;10(7):1137–1148. doi:10.1586/era.10.86. - DOI - PubMed
-
- Bruna J, González L, Miró J, Velasco R, Gil M, Tortosa A. Leptomeningeal carcinomatosis: prognostic implications of clinical and cerebrospinal fluid features. Cancer. 2009;115(2):381–389. doi:10.1002/cncr.24041. - DOI - PubMed
-
- Shapiro RS, Johanson CE, Boogera W. Treatment modalities for leptomeningeal metastases. Sem Oncol. 2009;36(4 Suppl 2):S46–54.6. doi:10.1053/j.seminoncol.2009.05.006. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
